What should be the second step of the who pain ladder?
Thus, the second step of the updated WHO pain ladder should specifically include fixed-dose combination analgesics. There are a number of FDA-approved oral, fixed-dose combination products (Table 2) 20-22 that are widely used in the treatment of a variety of pain syndromes. 23-25 Step 3: Strong Opioids and Adjuvant Agents
What is the four-step ladder for pain relief?
Such four-step ladder, as opposed to the 1986 “ladder”, reflects the advances in nonopioid modalities application for better pain relieving. The integrative medicine therapies can be adopted in each step for reducing or even stopping the use of analgesics to all types of pains.
What is the second step treatment for moderate pain?
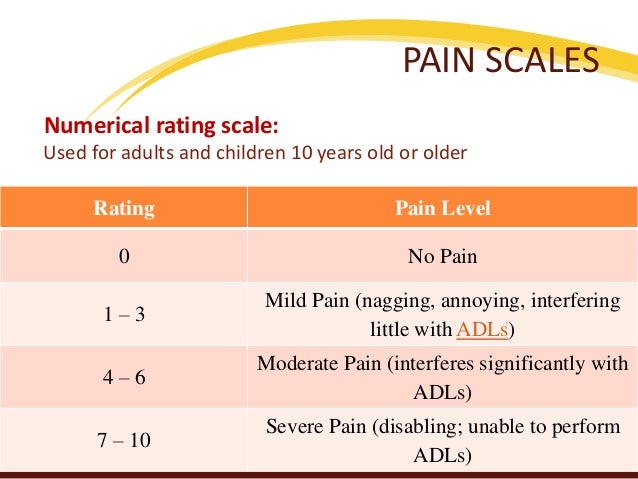
According to the WHO pain relief ladder, a second-step treatment (for moderate pain) is: Oxycodone + aspirin Different types of pain scales are used to determine the intensity of patient pain.
Does the who pain ladder work?
While the WHO pain ladder is imperfect, the same could be said of any one-size-fits-all approach to pain. But the brilliance of the pain ladder is that it works and works well most of the time when used as intended.
WHO pain relief ladder a second step treatment for moderate pain is?
Second step. Moderate pain: weak opioids (hydrocodone, codeine, tramadol) with or without non-opioid analgesics, and with or without adjuvants. Third step.
What is the 2 step method to pain management?
Patients generally start on Step 1 of the ladder (paracetamol). As pain increases or is not well controlled on this, they progress to Step 2 which involves a stronger pain killer (weak opioid such as codeine).
What is the WHO 3 step analgesic ladder?
Its three steps are: Step 1 Non-opioid plus optional adjuvant analgesics for mild pain; Step 2 Weak opioid plus non-opioid and adjuvant analgesics for mild to moderate pain; Step 3 Strong opioid plus non-opioid and adjuvant analgesics for moderate to severe pain.
WHO analgesic ladder explained?
The 1986 version of the WHO analgesic ladder proposes that treatment of pain should begin with a nonopioid medication (Figure 1). If the pain is not properly controlled, one should then introduce a weak opioid. If the use of this medication is insufficient to treat the pain, one can begin a more powerful opioid.
What is the treatment of pain?
pain medicines. physical therapies (such as heat or cold packs, massage, hydrotherapy and exercise) psychological therapies (such as cognitive behavioural therapy, relaxation techniques and meditation) mind and body techniques (such as acupuncture)
What are the 3 types of analgesics?
There are three broad categories of analgesic medications: (1) nonopioid analgesics, which includes the nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, dipyrone, and others; (2) a diverse group of drugs known as the "adjuvant analgesics," which are defined as "drugs that have primary indications other ...
What is the first line treatment for neuropathic pain?
First line treatment in neuropathic pain is pregabalin, gabapentin, duloxetine and amitriptyline. Second choice drugs are topical capsaicin and lidocaine, which can also be considered as primary treatment in focal neuropathic pain. Opioids are considered as third choice treatment.
What is an example of adjuvant analgesic?
Commonly used drugs in this class include: baclofen (Lioresal), carisoprodol (Soma), cyclobenzaprine (Flexeril), diazepam (Valium), methocarbamol (Robaxin), orphenadine (Norflex), metaxalone (Skelaxin), and tizanidine (Zanaflex).
Which drug is analgesic?
Analgesics are a class of medications designed specifically to relieve pain. They include acetaminophen (Tylenol), which is available over the counter (OTC) or by prescription when combined with another drug, and opioids (narcotics), which are only available by prescription.
Where is Nefopam on the analgesic ladder?
Where does nefopam fit in the pain ladder? Being classed as a non-opioid, nefopam technically fits into all stages of the pain ladder. In practice however, it is more commonly used in step 2 or 3 of the ladder, alongside paracetamol and a weak opioid such as codeine.
What is the WHO analgesic ladder?
The WHO analgesic ladder was a strategy proposed by the World Health Organization (WHO), in 1986, to provide adequate pain relief for cancer patients .[1] . The analgesic ladder was part of a vast health program termed the WHO Cancer Pain and Palliative Care Program aimed at improving strategies for cancer pain management ...
What is the first step in pain management?
First step. Mild pain: non-opioid analgesics such as nonsteroidal anti-inflammatory drugs (NSAIDs) or acetaminophen with or without adjuvants . Second step. Moderate pain: weak opioids (hydrocodone, codeine, tramadol) with or without non-opioid analgesics, and with or without adjuvants .
What is the strongest analgesic?
For acute pain, the strongest analgesic (for that intensity of pain) is the initial therapy and later toned down, whereas, for chronic pain, employing a step-wise approach from bottom to top. However, clinicians should also provide de-escalation in the case of chronic pain resolution. Issues of Concern.
What is the WHO ladder?
The WHO analgesic ladder was a strategy proposed by the World Health Organization (WHO), in 1986, to provide adequate pain relief for cancer patients .[1] .
What is the third step of opioids?
Third step. Severe and persistent pain: potent opioids (morphine, methadone, fentanyl, oxycodone, buprenorphine, tapentadol, hydromorphone, oxymorphone) with or without non-opioid analgesics, and with or without adjuvants . The term adjuvant refers to a vast set of drugs belonging to different classes.
How can clinicians dynamically manage pain?
Through this approach, clinicians can dynamically manage pain by combining several pharmacologic and non-pharmacologic strategies according to the physiopathology of pain, pain features, and the complexity of symptoms, the presence of comorbidity, and the physiopathological factors, and the social context.
Is there a standardized dosage for pain?
This method presupposes is that there is no standardized dosage in the treatment of pain. Probably, it is the biggest challenge in pain medicine, as the dosology must be continuously adapted to the patient, balancing analgesic desired effects and the possible occurrence of side effects.
What is the Pain Ladder?
Pain ladder. "Pain ladder", or analgesic ladder, was created by the World Health Organization (WHO) as a guideline for the use of drugs in the management of pain. Originally published in 1986 for the management of cancer pain, it is now widely used by medical professionals for the management of all types of pain .
When was the first step drug for cancer pain first published?
Originally published in 1986 for the management of cancer pain, it is now widely used by medical professionals for the management of all types of pain . The general principle is to start with first step drugs, and then to climb the ladder if pain is still present.
What is the best treatment for neuropathic pain?
Tricyclic antidepressants, class I antiarrhythmics, or anticonvulsants are the drugs of choice for neuropathic pain. Up to 90 percent of cancer patients, immediately preceding death, use such adjuvants. Many adjuvants carry a significant risk of serious complications.
Can analgesics reduce pain?
Not all pain yields completely to classic analgesics, and drugs that are not traditionally considered analgesics, but which reduce pain in some cases, such as steroids or bisphosphonates, may be employed concurrently with analgesics at any stage.
What is the WHO analgesic ladder?
The WHO analgesic ladder was a strategy proposed by the World Health Organization (WHO), in 1986, to provide adequate pain relief for cancer patients. [1] . The analgesic ladder was part of a vast health program termed the WHO Cancer Pain and Palliative Care Program aimed at improving strategies for cancer pain management ...
Why was the analgesic ladder designed?
[14] The lack of proper knowledge of drugs, underdosing and wrong timing of drugs, fear of addiction in patients, and lack of public awareness are severe limitations that limit the proper implementation of the strategy. [15]
What is the first step in pain management?
First step. Mild pain: non-opioid analgesics such as nonsteroidal anti-inflammatory drugs (NSAIDs) or acetaminophen with or without adjuvants. Second step. Moderate pain: weak opioids (hydrocodone, codeine, tramadol) with or without non-opioid analgesics, and with or without adjuvants. Third step.
What is the third step of opioids?
Third step. Severe and persistent pain: potent opioids (morphine, methadone, fentanyl, oxycodone, buprenorphine, tapentadol, hydromorphone, oxymorphone) with or without non-opioid analgesics, and with or without adjuvants. The term adjuvant refers to a vast set of drugs belonging to different classes.
What is the strongest analgesic?
For acute pain, the strongest analgesic (for that intensity of pain) is the initial therapy and later toned down, whereas, for chronic pain, employing a step-wise approach from bottom to top. However, clinicians should also provide de-escalation in the case of chronic pain resolution.
How can clinicians dynamically manage pain?
Through this approach, clinicians can dynamically manage pain by combining several pharmacologic and non-pharmacologic strategies according to the physiopathology of pain, pain features, and the complexity of symptoms, the presence of comorbidity, and the physiopathological factors, and the social context.
Is there a standardized dosage for pain?
This method presupposes is that there is no standardized dosage in the treatment of pain. Probably, it is the biggest challenge in pain medicine, as the dosology must be continuously adapted to the patient, balancing analgesic desired effects and the possible occurrence of side effects.
What is the purpose of the Baseline Pain Assessment?
This group of drugs is often used in lower doses as an adjuvant drug to treat chronic nerve pain by regulating the pain signals and increasing mood. Antidepressants.
What is the biological function of pain?
The biological function of pain is to warn the body of injury. The type of pain that properly serves this function is: Acute pain. Different types of pain scales are used to determine the intensity of patient pain.
Can you use placebo for pain?
Choose the correct statement about placebos and pain management: Placebos should not be used to treat pain. When assessing the functional goals, you are determining: What a person would like to be able to do if pain is managed. The preferred treatment plan for chronic pain is:
What is the second step of pain management?
Pain management promotes overall health and well-being. According to the WHO pain relief ladder, a second-step treatment (for moderate pain) is: Oxycodone + aspirin. Different types of pain scales are used to determine the intensity of patient pain.
Can you use placebos for pain?
Placebos should not be used to treat pain. Used for complex acute pain and chronic pain (including cancer pain), multidimensional pain scales measure: Intensity, location, and impact on activity and/or mood. Choose the true statement about the benefit of pain management:
Scope of Pain Problem
- Nine million new cases of cancer are reported each year, the majority of which occur in developing nations.⁴ Oncologists all over the world focus on disease management rather than pain control,⁵ with the result that much cancer pain is undertreated or entirely untreated. Concer…
A New Paradigm in Pain Management
- When the WHO first published their pain ladder in 1986, it offered guidance for clinicians around the world in treating cancer pain.¹ What made this simple diagrammatic ladder so enduring is the fact that it was intuitively understandable and could be immediately implemented anywhere in the world, including under-developed nations and regions with few pain specialists. A quarter centur…
Better Understanding of Pain Emerging
- As noted, today pain medicine has identified different mechanisms of pain (such as neuropathic, nociceptive, visceral) and recognizes that some pain syndromes can be multimodal—that is, primarily nociceptive pain can present with a neuropathic component. Most pain experts do not rely on the WHO pain ladder because it was not designed for highly complex cases, chronic non…
Deploying The Pain Ladder in Clinical Practice
- The first update to the WHO pain ladder we propose is not a new step, but rather guidance to clinicians that the pain ladder should be adapted to meet the needs of individual patients. Pain control must be individualized for optimal benefit. A study of cancer pain patients found that strict adherence to the WHO pain ladder resulted in inadequate analgesia in 39% of patients, but whe…
Discussion
- Pain is the most common reason patients seek medical care,⁴⁰ and most clinicians frequently treat patients with pain. The 1986 WHO pain ladder was extraordinarily successful in globally introducing a simple but effective care paradigm for patients dealing with cancer pain. With patients living longer with cancer and chronic pain, the clinical community needs to be reminde…
Conclusion
- Over a quarter century after its publication, the WHO pain ladder is still an influential and practical guide for clinicians around the world for the management of cancer pain. So successful has been this simple ladder diagram that it has been used to help guide analgesia for noncancer pain syndromes as well. While we applaud the simplicity and practicality of the WHO pain ladder, tod…