Medication
Treatment. Treatment for small bowel cancer depends on the type of cancer you have and its stage. Options might include: Surgery. Surgeons work to remove all of the small bowel cancer, when possible. If cancer affects a small portion of the small intestine, surgeons may remove only that section and rejoin the cut ends of the intestine.
Procedures
Small bowel cancer can be difficult to diagnose, and symptoms may be vague and caused by other conditions. Symptoms may include: abdominal (tummy) pain. unexplained weight loss. a lump in the abdomen. blood in the stools. change in bowel habit including diarrhoea, constipation or the feeling of incomplete emptying.
Therapy
Pancreatic neuroendocrine tumors (NETs) are classified by tumor grade, which describes how quickly the cancer is likely to grow and spread. Grade 1 (also called low-grade or well-differentiated) neuroendocrine tumors have cells that look more like normal cells and are not multiplying quickly.
Nutrition
With a child dying from cancer every 3 min and survival as low as 20% in many low-income and ... Despite risks of endocrine-system cancers such as those of the thyroid, pancreas, and neuroendocrine system being lower among this age group, survivors of ...
See more
What is the treatment for small bowel cancer?
What are the symptoms of small bowel cancer?
What is a Grade 1 neuroendocrine tumour?
What is the prognosis for neuroendocrine cancer?

Do you need to go through chemo for neuroendocrine cancer?
Chemotherapy uses anti cancer (cytotoxic) drugs to destroy neuroendocrine tumour (NET) cells. The drugs circulate throughout your body in the bloodstream. Chemotherapy isn't usually the first choice of treatment for NETs.
What is the survival rate of small cell neuroendocrine carcinoma?
Most people with SCLC are diagnosed when their cancer has spread beyond a single area that can be treated with radiotherapy (extensive stage). Between 20 and 40 out of every 100 people (between 20% and 40%) with limited stage SCLC survive for 2 years or more.
How long does it take for a neuroendocrine tumor to grow?
In general, it can take 3-5 years and even up to 10 or longer for carcinoid tumors to grow.
Can you live with neuroendocrine cancer?
Around 90 out of 100 people (around 90%) survive for 1 year or more. Around 89 out of every 100 people (around 89%) people survive for 5 years or more. This 5 year survival rate was taken from a European study that looked at 270 people diagnosed with a gut neuroendocrine tumour between 1984 and 2008.
How long can you live with neuroendocrine carcinoma?
The median survival duration was 41 months. The 1-, 3-, 5-, and 10-year overall survival rates for patients with NETs were 72.8%, 52.7%, 39.4%, and 18.1%, respectively.
Are neuroendocrine tumors life threatening?
Studies show that these types of tumors can potentially last a lifetime without causing symptoms or spreading. As a result, the survival rate—especially for neuroendocrine tumors that are diagnosed in early stages and properly treated—can be favorable.
Can neuroendocrine tumors spread to brain?
The incidence of brain metastases for neuroendocrine tumor (NET) is reportedly 1.5~5%, and the origin is usually pulmonary. A 77-year-old man presented to our hospital with headache and disturbance of specific skilled motor activities.
Are neuroendocrine tumors slow-growing?
Neuroendocrine tumours (NETs) are rare, small, slow-growing tumours most often originating in the gastrointestinal tract and lungs. They can also develop in the pancreas, ovaries, testes, and other areas of the neuroendocrine system.
Do neuroendocrine tumors cause pain?
In general, neuroendocrine tumor signs and symptoms might include: Pain from a growing tumor. A growing lump you can feel under the skin. Feeling unusually tired.
How long did Steve Jobs live after diagnosis?
After a delay of nine months after diagnosis, in 2004, Jobs opted for surgery. He died 7 years later. There has been widespread speculation about whether Jobs' decision to use CAM approaches hastened his death by postponing initiation of potentially life-prolonging conventional treatments (Grady, 2011).
What is the best treatment for neuroendocrine cancer?
In general, neuroendocrine tumor treatment options might include:Surgery. Surgery is used to remove the tumor. ... Chemotherapy. Chemotherapy uses strong drugs to kill tumor cells. ... Targeted drug therapy. ... Peptide receptor radionuclide therapy (PRRT). ... Medications to control excess hormones. ... Radiation therapy.
Where do neuroendocrine tumors metastasize?
The metastatic potential of NET was assessed. The liver was the most common site of metastasis (82% of patients with metastases), and the small intestine was the most common source of NET metastases.
How to treat neuroendocrine tumors?
In general, neuroendocrine tumor treatment options might include: Surgery. Surgery is used to remove the tumor. When possible, surgeons work to remove the entire tumor and some of the healthy tissue that surrounds it. If the tumor can't be removed completely, it might help to remove as much of it as possible.
What to do if neuroendocrine tumor releases hormones?
If your neuroendocrine tumor releases excess hormones, your doctor might recommend medications to control your signs and symptoms.
What tests can be done to determine if a tumor is producing hormones?
In general, tests might include: Physical exam. Your doctor may examine your body to better understand your signs and symptoms. He or she may feel for swollen lymph nodes or look for signs that a tumor is producing excess hormones. Tests to look for excess hormones.
How to cope with cancer?
Turn to family and friends for support. Stay connected to family and friends for support. It can be tough to talk about your diagnosis, and you'll likely get a range of reactions when you share the news. But talking about your diagnosis and passing along information about your cancer can help you cope — and so can the offers of practical help that often result.
Can neuroendocrine tumors spread to other parts of the body?
If there's a risk that your neuroendocrine tumor may have spread to other parts of your body, you might have additional tests to determine the extent of the cancer.
Does Mayo Clinic treat neuroendocrine tumors?
Our caring team of Mayo Clinic experts can help you with your neuroendocrine tumors-related health concerns Start Here
Is it stressful to be diagnosed with neuroendocrine tumors?
Being diagnosed with a neuroendocrine tumor can be stressful and overwhelming. With time, you'll find ways to cope with the distress and uncertainty. Until then, you may find that it helps to:
What is a small bowel neuroendocrine tumour?
Small bowel neuroendocrine tumours (NETs) are rare bowel tumours. They start in the neuroendocrine cells of the small bowel. They often develop slowly and don’t always have specific symptoms.
Which organs have neuroendocrine cells?
Neuroendocrine cells don’t form an actual organ. Instead, they are scattered throughout other organs like the oesophagus, stomach, pancreas, intestines, and lungs. They make hormones which control how our bodies work. The digestive system is large and has more neuroendocrine cells than any other part of the body.
How common are small bowel NETs?
Small bowel NETs are rare cancers. Around 4 out of 10 small bowel tumours (around 40%) are neuroendocrine tumours. Most NETs start somewhere in the digestive system (gut). And around 40 out of every 100 of these digestive system neuroendocrine tumours (around 40%) start in the small bowel.
What next?
You might be interested to read about the possible symptoms of small bowel NETs.
What is the bowel that connects to the colon called?
ileum (ill-ee-um) – the lower part, which connects to the large bowel (colon) Right at the end of the ileum, just before it joins to the colon, is a small pouch called the appendix. Small bowel NETs include any that develop in the ileum and the jejunum. Doctors group some NETs that develop in the duodenum with NETs that start in the pancreas.
Where is the appendix in the small bowel?
It is about 6 metres long, but it is folded up so that it fits inside the abdomen. Right at the end of the ileum, just before it joins to the colon, is a small pouch called the appendix. Small bowel NETs include any that develop in the ileum and the jejunum.
Can cancer cause a small bowel NET?
At the moment, no clear risk factors have been found that increase your chance of developing a small bowel NET. Having a family history of cancer is a risk factor for all types of NET including small bowel NETs. We have more information on family history and inherited cancer genes.
What are the factors that determine the treatment of a NET tumor?
These include the location of the tumor, whether it is functional or non-functional, and how advanced the disease is.
What is the treatment for NET?
NET treatment plans. Regardless of location, the preferred treatment for most NETs is surgery to remove the entire tumor. This may cure the patient. Most surgeries meant to cure NETs are performed on patients whose disease has not metastasized, or spread.
What tests are done to see if a tumor is growing?
With this approach, the patient undergoes regular tests, including blood, urine and imaging exams, to see if the tumor is growing. No treatments are given unless and until the disease progresses. This is a popular approach for older patients who might find surgery or other therapies difficult to bear.
What do cancer cells need to survive?
This happens on a cellular level. Cancer cells need specific molecules (often in the form of proteins) to survive, multiply and spread. These molecules are usually made by the genes that cause cancer, as well as the cells themselves.
How can cancer be prevented?
Many cancers can be prevented with lifestyle changes and regular screening.
Can a surgeon remove a tumor?
If the surgeon cannot remove the entire tumor, only part of it may be removed in order to help treat a patient’s tumor-related symptoms. The patient’s surgical options will depend on the tumor’s location. The procedures are essentially identical to surgeries for other types of tumors at that site. For example, if a patient has lung cancer, ...
Can a tumor be removed through surgery?
In some cases, though, patients whose disease has metastasized can be effectively cured by surgery that removes the primary tumor and the metastases. For the vast majority of patients, it is not possible to remove the entire tumor through surgery.
What is the most common treatment for a NET in the small and large intestine?
Small intestine/large intestine (colon). Surgery to remove the tumor, surrounding tissue, and lymph nodes is the most common treatment for a NET in the small and large intestine.
When does treatment start for a tumor?
Treatment usually only begins if the tumor shows signs of growing or spreading.
What is the treatment for a tumor in the liver?
Radioembolization. This form of radiation therapy involves the use of tiny beads made of glass or resin that contain low levels of a radioactive material called yttrium-90. The beads are put into the blood vessel that sends blood to the tumor in the liver. The beads then become stuck in the liver and deliver the radiation directly to the tumor. This treatment avoids exposing other areas of the body to radiation. There are 2 FDA-approved methods of radioembolization: SIR-Spheres and TheraSphere.
How to remove a NET of the stomach?
Stomach. A localized NET of the stomach can often be completely removed through an endoscope. A tumor larger than 2 cm is removed with a margin of surrounding stomach tissue through an incision, or cut, in the abdomen. Treatment plans for NETs of the stomach also depend on whether they are associated with the secretion of gastrin and if an endoscopy finds inflammation of the stomach cells, called atrophic gastritis. This information helps determine the specific subtype of the tumor: type 1, 2, or 3. This can be a complicated diagnosis, and you are recommended to work with your gastroenterologist or oncologist on making this diagnosis and selecting the best treatment.
What is it called when you have no surgery?
If no surgery is possible, it is called an “inoperable” tumor. In these situations, the doctor will recommend another type of treatment. People who have carcinoid syndrome are at risk of experiencing a carcinoid crisis during surgery and other procedures (see Symptoms and Signs ).
How does chemotherapy kill cancer cells?
Chemotherapy is the use of drugs to destroy cancer cells, usually by keeping the cancer cells from growing, dividing, and making more cells. Chemotherapy for a GI tract NET is most often used when the tumor has spread to other organs or is causing severe symptoms.
What is standard of care for GI tract?
This section explains the types of treatments that are the standard of care for a GI tract NET. “Standard of care” means the best treatments known. When making treatment plan decisions, you are also encouraged to consider clinical trials as an option.
What is a neuroendocrine tumor?
Neuroendocrine tumors (NETs) are a diverse group of neoplasms that arise from endocrine cells throughout the body. Though they share common histologic and biochemical properties, the natural history, malignant potential, and treatment of these tumors can vary dramatically.
What is a small bowel NET tumor?
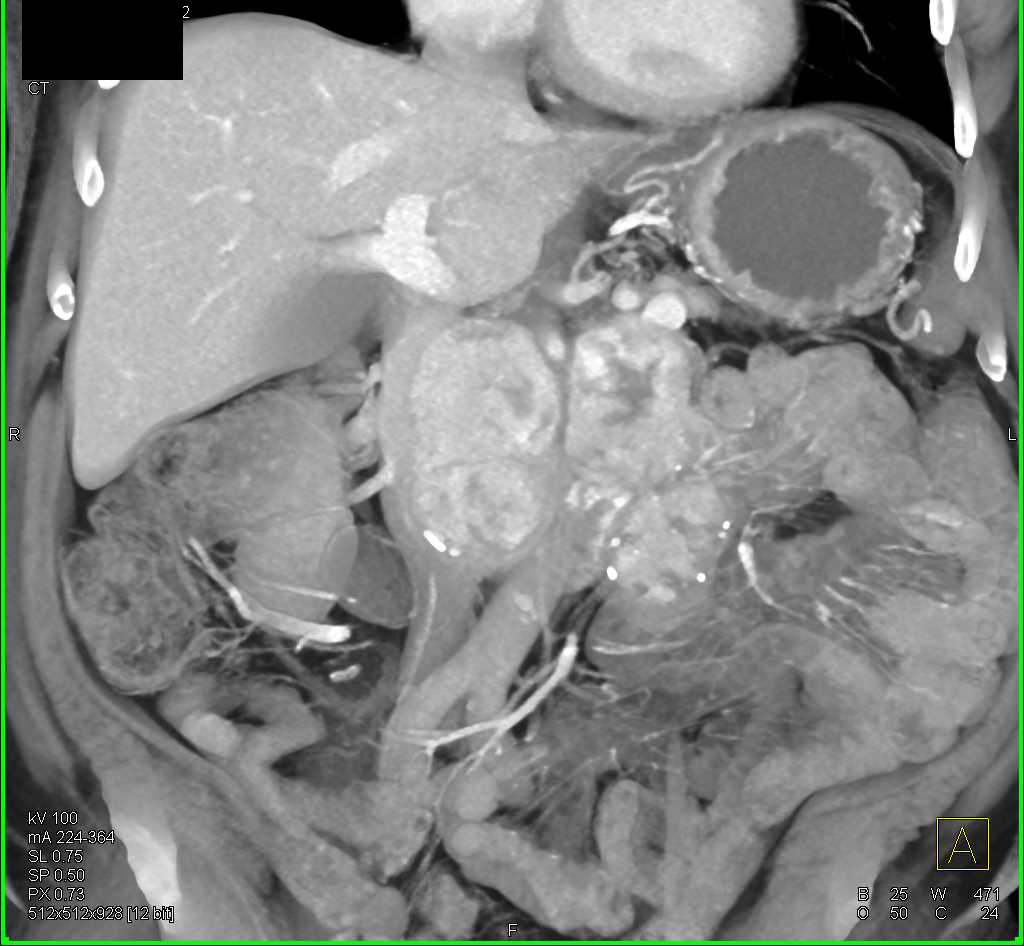
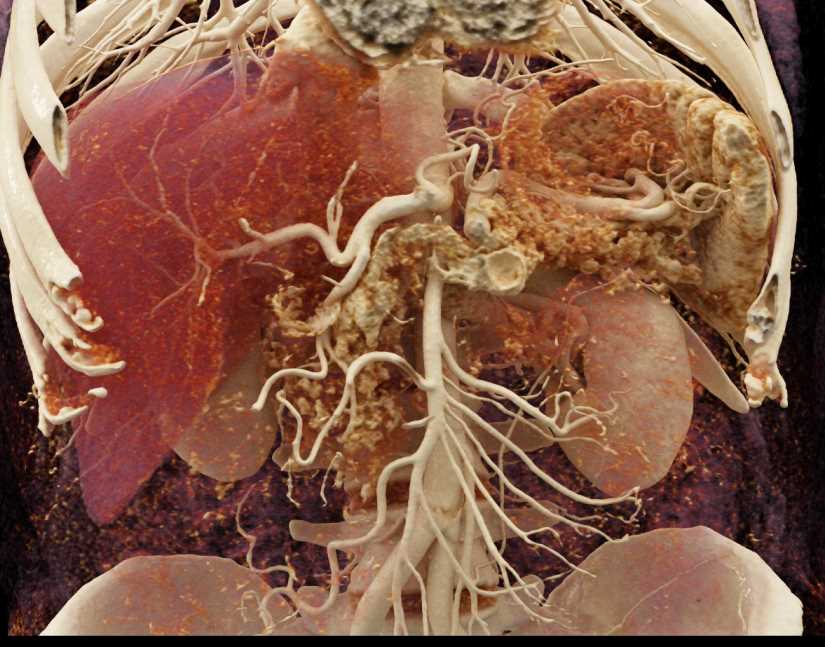
Although small bowel NET primary tumors are typically small, they have a tendency to induce a pronounced fibrotic reaction in the mesentery and often are accompanied by a mesenteric mass that represents enlarged regional lymph nodes ( Fig 1 ). 23 Fibrosis associated with small bowel NETs was first described by Moertel et al 24 in 1961 and leads to significant morbidity and mortality as a result of intestinal obstruction and ischemia. 23 - 27 Patients may present with episodic, crampy abdominal pain characteristic of recurrent partial bowel obstruction or with complete obstruction that requires emergent surgery; in some reports nearly half of patients with small bowel NETs present with obstructive symptoms. 10, 25
What are the biochemical markers of small bowel NETs?
Small bowel NETs secrete several biochemical markers that can be measured as part of the diagnostic workup of a patient with symptoms suggestive of the carcinoid syndrome or as biochemical surveillance of those with an established diagnosis. Chromogranin A is an acidic glycoprotein that is secreted by a wide variety of NETs, including nonfunctional tumors (ie, those not associated with a hormonal syndrome). 10, 19 Chromogranin A is a sensitive and specific marker for NETs that correlates with both tumor volume and prognosis; however, practitioners should be aware that a number of conditions, including proton pump inhibitor therapy, severe hypertension, or renal failure, can cause falsely elevated levels. 18, 30, 31
How long do you survive a metastatic small bowel NET?
23 Numerous retrospective studies have demonstrated improved survival and symptomatic control with resection of nodal 25, 27 and hepatic 22, 63, 64 metastases: 5-year overall survival rates varied from 65% to 88%. These procedures are rarely curative, and 5- and 10-year recurrence rates are 95% and 99%, respectively. 64 This high recurrence rate shifts the emphasis from cure to debulking, a notion which also is supported by the lack of survival benefit associated with R0 versus R1 or R2 resection. 63, 64 Historically, hepatic debulking has been attempted only when resection of 90% of the metastases was deemed feasible, but recent studies have found equivalent survival with a threshold of 70% cytoreduction. 22, 63 Adoption of this lower debulking threshold—along with the use of parenchyma-sparing surgical techniques, which include wedge resection, enucleation, and intraoperative radiofrequency or microwave ablation—allows for as many as 76% of patients to undergo hepatic debulking. 22 In contrast, when patients are selected on the basis of the feasibility of achieving 90% cytoreduction, less than 25% will undergo surgery. 22, 23 Contraindications to surgery are debated, but, in general, patients with greater than 50% liver replacement, numerous small metastases, poor performance status, liver dysfunction, or high-grade disease should not be considered for hepatic debulking. 23 Resection of the primary tumor, which can be accomplished at the same time as hepatic cytoreduction, should be performed when feasible to avoid potential future complications from an obstructing small bowel lesion or mesenteric mass and to prevent carcinomatosis or the development of additional liver metastases. 23 Even if a patient’s hepatic metastases are unresectable, resection of the primary appears to improve survival. 25, 29 In patients who are ineligible for hepatic debulking, liver transplantation may offer the potential for curative resection and appears to improve survival. 65, 66 Eligibility for transplantation is determined by the Milan-NET criteria, 66 but the potential benefits of this extensive procedure must be weighed against the national shortage of grafts. 65 Finally, cholecystectomy should be performed at the time of surgery for metastatic small bowel NETs because of the high incidence of gallstones in patients who receive somatostatin analogs. 23
What are the symptoms of carcinoid syndrome?
10, 17, 18 Other clinical signs variably attributed to the carcinoid syndrome include telangiectasias, cyanosis, pellagra-like dermatitis, arthritis, myopathy, edema, and ascites, though it should be noted that these frequently are sequela of hepatic tumor replacement or carcinoid heart disease rather than excess hormone secretion. 10, 16 - 18 The syndrome is caused by the secretion of hormones, including serotonin, neurokinin A, histamine, and others. 10, 19 In tumors confined to the small bowel and regional lymph nodes, most of these hormones enter the portal circulation and are inactivated by the liver; consequently, the classical carcinoid syndrome is rarely seen in the absence of metastatic disease. 18, 20 Despite the historical use of the term “carcinoid” to refer to both NETs and the carcinoid syndrome, most patients present with nonspecific abdominal pain rather than with symptoms of excess hormone secretion. 10, 18, 21, 22 Because of the relatively low incidence, the lack of physician awareness, and the vague presenting symptoms related to small bowel NETs, patients with these small bowel NETs often experience long delays in diagnosis. 15, 19 The reported duration of symptoms that precede diagnosis varies considerably in the literature from a median of 4.3 months at a large academic institution 21 to as long as a median of 9.2 years. 19
What is the best treatment for pancreatic NETs?
Cytotoxic chemotherapy is well established in the treatment of pancreatic NETs but plays a limited role in the treatment of well-differentiated small bowel NETs. 57 Streptozocin, often used in combination with fluorouracil or doxorubicin, is approved for use in pancreatic NETs, but its efficacy against small bowel NETs is not established, and it is associated with significant toxicity. 57, 58 Other chemotherapeutic options include dacarbazine, oxaliplatin plus capecitabine or fluorouracil, and irinotecan-based therapy. 58 Strong evidence to favor any one chemotherapeutic regimen compared with another for small bowel NETs is lacking, and most studies identified in a 2016 meta-analysis were nonrandomized and included NETs from a variety of primary sites. 57 Interferon alfa, which was used as a control arm in three randomized trials in the aforementioned meta-analysis, is thought to inhibit tumor growth and improve symptom control on the basis of a number of small prospective and retrospective studies, but it is not widely used at this time because of the lack of high-quality evidence and an unfavorable adverse effect profile. 31, 57 In recent years, the combination of capecitabine and temozolomide has been demonstrated to yield response rates from 30% to 70% in pancreatic NETs. 59 Data to support the use of capecitabine and temozolomide in small bowel NETs is based on small numbers of patients in retrospective studies, and objective response rates in nonpancreatic NETs are significantly lower—ranging from 14% in a heavily pretreated population to 42%. 60, 61 Despite this, the convenient oral route of administration and favorable adverse effect profile make capecitabine and temozolomide a reasonable second- or third-line option in patients with progressive small bowel NETs.
How to treat liver metastases?
In addition to surgical debulking, less invasive methods, such as hepatic artery embolization and percutaneous liver ablation, can be used to treat small bowel NET liver metastases. Embolization involves the injection of particles into the hepatic artery or its branches to occlude blood flow to the liver metastases, which are supplied primarily by the hepatic arteries. 67 It can be performed with inert particles (bland), beads along with a chemotherapeutic agent (chemoembolization), or 90 Y-conjugated beads (radioembolization). To date, no single therapy has shown clear superiority. 20, 67 Symptomatic response rates to hepatic artery embolization range from 39% to 95%. 67 Percutaneous liver ablation involves the insertion of a microwave or radiofrequency probe into hepatic metastases under image guidance and subsequent heating of the lesions to induce necrosis. High-quality evidence to support the use of percutaneous ablation is lacking. Although reported complication rates are low and symptomatic response rates are favorable, many series pool the results from operative and percutaneous ablative procedures, which makes interpretation difficult. 68 For patients with liver-dominant disease who are not surgical candidates, both hepatic artery embolization and percutaneous ablation may be considered for disease control. 20, 31
How to treat a recurrent tumor?
Often the treatment plan will include the treatments described above, such as surgery, chemotherapy, and radiation therapy, but they may be used in a different combination or given at a different pace. Your doctor may suggest clinical trials that are studying new ways to treat this type of recurrent tumor. Whichever treatment plan you choose, palliative care will be important for relieving symptoms and side effects.
What is the procedure to remove a tumor?
Surgery. Surgery is the removal of the tumor and some surrounding healthy tissue during an operation. A surgical oncologist is a doctor who specializes in cancer surgery. Completely removing the entire tumor is the standard treatment, when possible.
What tests are done to detect a tumor?
With this approach, the tumor is closely monitored with regular tests, which may include: Imaging tests, usually CT scans or sometimes MRI scans (see Diagnosis) Blood tests. Physical examinations.
How does chemotherapy destroy cancer cells?
Chemotherapy is the use of drugs to destroy cancer cells, usually by keeping the cancer cells from growing, dividing, and making more cells.
How is medication used to treat cancer?
Medication may be given through the bloodstream to reach cancer cells throughout the body. When a drug is given this way, it is called systemic therapy . Medication may also be given locally, which is when the medication is applied directly to the cancer or kept in a single part of the body.
Who prescribes a syringe for cancer?
This type of medication is generally prescribed by a medical oncologist, a doctor who specializes in treating cancer with medication.
Can you cure a NET tumor?
Debulking surgery removes as much of the tumor as possible and may provide some relief from symptoms, but it generally does not cure a NET.
What is the newest treatment for neuroendocrine tumors?
The newest option is a type of systemic radiation called peptide receptor radionuclide therapy, or PRRT. The vast majority of neuroendocrine tumors will have specific hormone receptors, so instead of giving patients the hormone therapy itself, ...
How to tell if a tumor is neuroendocrine?
We tend to see neuroendocrine symptoms in two categories: 1 Hormonal: These include severe diarrhea, severe gastric ulcers, or uncontrolled blood sugar that respond poorly to treatment. The hormones produced can vary depending on the place in the body where the tumor originates. 2 Mechanical: These relate to the function of one part of the body, such as a small bowel obstruction, or pain in a particular place. These symptoms occur because the tumor is physically pushing on another structure.
How long does it take for a neuroendocrine tumor to get worse?
Many patients with neuroendocrine tumors have hormonal symptoms that get progressively worse. So, they can experience symptoms for an average of five to seven years before finally receiving a neuroendocrine tumor diagnosis.
What are the symptoms of neuroendocrine tumors?
We tend to see neuroendocrine symptoms in two categories: Hormonal: These include severe diarrhea, severe gastric ulcers, or uncontrolled blood sugar that respond poorly to treatment. The hormones produced can vary depending on the place in the body where the tumor originates.
What is the name of the tumor that involves both nerve cells and hormones?
While the name “neuroendocrine” implies that these tumors involve both nerve cells and hormones, they are mainly thought to come from endocrine cells. The “neuro-” is more of a quirk of history.
Where do neuroendocrine tumors occur?
They are distributed throughout the body, but the most common places for tumors to develop from them are in the lungs, small intestines and pancreas.
Can neuroendocrine tumors be treated?
But even when a neuroendocrine tumor has spread, surgery can still be useful in certain circumstances.
Diagnosis
Treatment
Clinical Trials
Coping and Support

Specialist to consult
Preparing For Your Appointment