The WHO 3-step ladder was devised in 1982 and officially adopted in 1986.¹⁻⁶ Although almost 30 years have passed since its adoption, it remains the pain treatment standard. It is not a specific opioid guideline but a template that provides a practical roadmap for pain treatment.
Who analgesic pain ladder?
· The original ladder mainly consisted of three steps[4]: First step. Mild pain: non-opioid analgesics such as nonsteroidal anti-inflammatory drugs (NSAIDs) or acetaminophen with... Second step. Moderate pain: weak opioids (hydrocodone, codeine, tramadol) with or without non-opioid analgesics, and... ...
Who 3 step analgesic ladder?
By the ladder: If pain occurs there should be prompt administration of drugs in the following order: • non-opiods (e. g. acetaminophen) • as necessary, mild opiods (e. g. codeine) • then strong opiods (e. g. morphine or hydromorphone) until the patient is free of pain. Drug selection should be appropriate to the severity of the pain.
Who pain scale ladder?
· Its three steps are: Step 1 Non-opioid plus optional adjuvant analgesics for mild pain; Step 2 Weak opioid plus non-opioid and adjuvant analgesics for mild to moderate pain; Step 3 Strong opioid plus non-opioid and adjuvant analgesics for moderate to severe pain.
Is the who analgesic ladder still valid?
The opioid epidemic challenges current attitudes toward pain management and necessitates the reexamination of the World Health Organization (WHO) 3-step analgesic ladder, introduced in 1986 for cancer pain management. Surgical treatment of pain is a logical extension of the original guideline, which is often absent in conversations with patients about treatment options for …

What is the pain ladder technique?
By the ladder: If pain occurs there should be prompt administration of drugs in the following order: • non-opiods (e. g. acetaminophen) • as necessary, mild opiods (e. g. codeine) • then strong opiods (e. g. morphine or hydromorphone) until the patient is free of pain.
WHO pain relief ladder second step treatment is?
Second step. Moderate pain: weak opioids (hydrocodone, codeine, tramadol) with or without non-opioid analgesics, and with or without adjuvants. Third step.
WHO analgesic ladder explained?
The 1986 version of the WHO analgesic ladder proposes that treatment of pain should begin with a nonopioid medication (Figure 1). If the pain is not properly controlled, one should then introduce a weak opioid. If the use of this medication is insufficient to treat the pain, one can begin a more powerful opioid.
What pain control method is recommended by the WHO?
A New Paradigm in Pain Management The WHO pain ladder (Figure 1) describes pain in terms of intensity and recommends that analgesics be prescribed starting at Step 1 (nonopioid analgesics, such as acetaminophen or non-steroidal anti-inflammatory drugs [NSAIDs]).
Is gabapentin an opioid?
Gabapentin is not a narcotic. It's not classified as a controlled substance in most states. (Kentucky, West Virginia, Michigan, Tennessee, and Virginia have reclassified gabapentin as a Schedule V controlled substance). Gabapentin is not an opioid.
What are the different types of pain?
The five most common types of pain are:Acute pain.Chronic pain.Neuropathic pain.Nociceptive pain.Radicular pain.
What is pain according to who?
The World Health Organisation defines pain as “an unpleasant sensory or emotional experience associated with actual or potential tissue damage, or described in terms of such damage”.
What is an example of adjuvant analgesic?
Commonly used drugs in this class include: baclofen (Lioresal), carisoprodol (Soma), cyclobenzaprine (Flexeril), diazepam (Valium), methocarbamol (Robaxin), orphenadine (Norflex), metaxalone (Skelaxin), and tizanidine (Zanaflex).
What is the difference between analgesic and anesthetic?
Analgesia is the relief of pain without the loss of consciousness or sensation using analgesics (e.g., Aspirin, Carprofen, etc.). Anesthesia, on the other hand, is the loss of physical sensation with or without loss of consciousness using anesthetics (e.g., Ketamine, Propofol, Isoflurane, etc.).
What is the preferred treatment plan for chronic pain?
Recommendation Summary. Narration Text: Nonopioid medications and nonpharmacologic treatments are preferred for chronic pain. Providers should consider opioid therapy only if expected benefits for both pain and function are anticipated to outweigh risks to the patient.
What is around the clock medication?
Shestock/Blend Images/Getty Images. ATC stands for "around-the-clock." Around-the-clock (ATC) medication is defined as medication that is given at regularly scheduled intervals throughout the day. This can include a dose during the night. Around-the-clock dosing is common for opioid medication to manage pain.
What is the treatment of pain?
pain medicines. physical therapies (such as heat or cold packs, massage, hydrotherapy and exercise) psychological therapies (such as cognitive behavioural therapy, relaxation techniques and meditation) mind and body techniques (such as acupuncture)
What are the steps of the Pain Ladder?
Its simple, progressive steps of 1) anti-inflammatory agents, 2) weak opioids, and 3) strong opioids is still fundamentally sound. In this article, Pergolizzi and Raffa present a thoughtful and detailed set of recommendations to modify the 3-step process. No doubt all of us have some thoughts about modifying the “WHO Pain Ladder,” based on the many new physical, interventional, and pharmacologic measures that have come forward since 1986. My message is that too many purveyors of potent opioid pharmaceuticals and invasive interventions have promoted and championed the use of these therapies, which have well-known complications, without first attempting regimens that are less onerous. Practical Pain Management desires that all pain practitioners make 2014 a year in which they develop and practice a “WHO Pain Ladder” protocol that is modified with some new measures to give our patients their best chance at a wide range of safe alternatives before resorting to potent opioids and invasive interventions.
Why add a fourth step to the pain ladder?
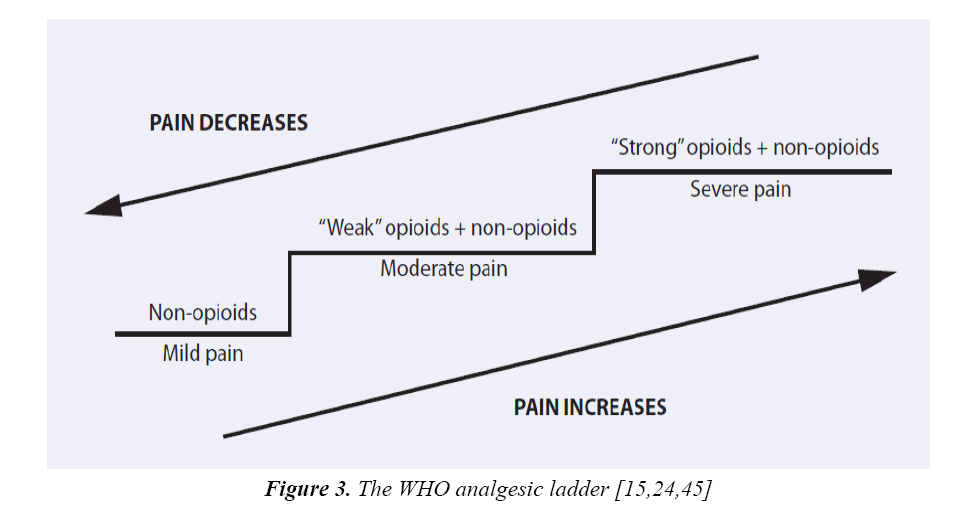
Retaining the use of pain intensity as the differentiator between steps, a fourth step could be added to the original pain ladder to accommodate very severe pain, such as occurs in the palliative setting in certain patients with advanced, particularly egregious forms of cancer. Pain specialists treat “very severe” noncancer pain as well. Severe to very severe pain may not respond to conventional pharmacologic treatment and may require intervention. This proposed change reflects modern clinical practice and our growing understanding of pain syndromes (Figure 3).
When was the pain ladder first published?
When the WHO first published their pain ladder in 1986 , it offered guidance for clinicians around the world in treating cancer pain. 1 What made this simple diagrammatic ladder so enduring is the fact that it was intuitively understandable and could be immediately implemented anywhere in the world, including under-developed nations and regions with few pain specialists. A quarter century later, the use of the WHO pain ladder still offers effective and cost-effective pain relief for patients suffering from cancer pain, even those near end of life.
What is the first step in pain management?
Step 1: Nonopioid Analgesics. Nonopioid analgesics include acetylsalicylic acid, acetaminophen, and selective and non-selective NSAIDs. The original WHO pain ladder states that adjuvant agents may be included with these nonopioid agents, but it does not name those agents.
Can cancer patients have breakthrough pain?
Pain may begin as severe; this is not unusual for cancer patients. More over, cancer patients frequently experience breakthrough pain, which can take a patient from persistent mild pain to very severe pain in a matter of moments. The original pain ladder would leave breakthrough pain patients without adequate analgesia.
Is morphine the gold standard?
There are good reasons for this selection: oral morphine is familiar, readily available, and inexpensive. Indeed, oral morphine is more or less the “gold standard” against which other opioid analgesics are measured. 26.
What is step 3 in cancer treatment?
Thus, when clinically appropriate and available, Step 3 may include “loose dose” combination therapy with a variety of other agents. Revising the third step to name some adjuvant medications may help clinicians be mindful of multimodal therapies that can be particularly beneficial in cancer pain.
What is the WHO 3-step analgesic ladder?
The opioid epidemic challenges current attitudes toward pain management and necessitates the reexamination of the World Health Organization (WHO) 3-step analgesic ladder, introduced in 1986 for cancer pain management. Surgical treatment of pain is a logical extension of the original guideline, which is often absent in conversations with patients about treatment options for their pain and consequentially underutilized. However, with concerns growing regarding opioid use, a shift in the stepwise approach of the WHO analgesic ladder in an age of developing technology and surgical offerings could have profound implications for patients and public health. Surgical interventions potentially provide a long-term, cost-effective management strategy to reduce opioid use. This review canvasses surgical options, highlights literature on failed back surgery syndrome and spinal cord stimulation and reconsiders the current ladder approach to pain management.
What is the 3 step ladder?
Presented in 1986, the World Health Organization (WHO) analgesic ladder provided a framework for the stepwise medical management of cancer-related pain. 1 This 3-step ladder begins with nonopioid analgesics with or without nonpharmacological approaches for mild pain, continues with weak opioid medications (eg, codeine) with or without nonopioid analgesics and adjuvants for mild-to-moderate pain, and progresses to strong opioids (eg, oxycodone) with or without nonopioid analgesics and adjuvants for moderate-to-severe pain. 1 The American Pain Society’s identification of pain as the “fifth vital sign” in 1995 portended the increased importance of not only adequate treatment of pain in patients but also education of health care professionals. 2, 3 Eventually, a modified version of the 3-step ladder placed interventional pain management as a fourth step. 4, 5 Development of this algorithmic approach aimed to control refractory or intractable pain in both an efficient and a safe manner, providing a rational and balanced method to maximize pain relief while minimizing side effects and risks.
Is surgery a final step in pain management?
Despite advances, surgical treatments remain a final step in pain management, typically after all other approaches fail. 37 With concerns growing regarding complications of opioid use in an age of developing technology and surgical offerings, a paradigm shift in pain management away from the WHO analgesic ladder toward earlier surgical intervention could have profound implications for patients and public health. Over time, surgical procedures have become more precise, less invasive, and better understood and recognized by both patients and their physicians. The ethical dilemma of beneficence vs nonmaleficence is not limited to weighing the advantages and risks of surgery alone. The risks of surgery avoidance should also be considered, given that medical (“conservative”) treatments can cause tolerance, dependence, or clinical side effects, as seen with most analgesic regimens, opioid or otherwise. The possibility of long-term pain relief and associated increase in functionality and improvement in quality of life justifies surgery as an earlier treatment option, perhaps before opioids are introduced.
Is neuromodulation reversible?
Each modality has advantages and disadvantages. Neuromodulation, both chemical and electrical, tends to be reversible, adjustable, testable, and nondestructive. It also provides patients with real or perceived ability to control the treatment using dedicated remote controllers.

Introduction

Scope of Pain Problem
- Nine million new cases of cancer are reported each year, the majority of which occur in developing nations.4 Oncologists all over the world focus on disease management rather than pain control,5 with the result that much cancer pain is undertreated or entirely untreated. Concern over palliative patients dying in severe (and potentially manageable) pain has been recognized a…
A New Paradigm in Pain Management
- When the WHO first published their pain ladder in 1986, it offered guidance for clinicians around the world in treating cancer pain.1What made this simple diagrammatic ladder so enduring is the fact that it was intuitively understandable and could be immediately implemented anywhere in the world, including under-developed nations and regions with few pain specialists. A quarter centur…
Better Understanding of Pain Emerging
- As noted, today pain medicine has identified different mechanisms of pain (such as neuropathic, nociceptive, visceral) and recognizes that some pain syndromes can be multimodal—that is, primarily nociceptive pain can present with a neuropathic component. Most pain experts do not rely on the WHO pain ladder because it was not designed for highly complex cases, chronic non…
Deploying The Pain Ladder in Clinical Practice
- The first update to the WHO pain ladder we propose is not a new step, but rather guidance to clinicians that the pain ladder should be adapted to meet the needs of individual patients. Pain control must be individualized for optimal benefit. A study of cancer pain patients found that strict adherence to the WHO pain ladder resulted in inadequate analgesia in 39% of patients, but whe…
Discussion
- Pain is the most common reason patients seek medical care,40 and most clinicians frequently treat patients with pain. The 1986 WHO pain ladder was extraordinarily successful in globally introducing a simple but effective care paradigm for patients dealing with cancer pain. With patients living longer with cancer and chronic pain, the clinical community needs to be reminde…
Conclusion
- Over a quarter century after its publication, the WHO pain ladder is still an influential and practical guide for clinicians around the world for the management of cancer pain. So successful has been this simple ladder diagram that it has been used to help guide analgesia for noncancer pain syndromes as well. While we applaud the simplicity and practicality of the WHO pain ladder, tod…