
Who treatment guidelines for drug- resistant tuberculosis?
1. Garlic...
2. Bananas...
3. Drumstick...
4. Indian Gooseberry...
5. Oranges...
6. Custard Apple...
7. Black Pepper...
8. Walnuts...
Learn More...Who found a cure to TB?
The present WHO Consolidated Guidelines on Tuberculosis, Module 4: Treatment - Drug-Resistant Tuberculosis Treatment includes a comprehensive set of WHO recommendations for the treatment and care of DR-TB. The document includes two new recommendations, one on the composition of shorter regimens and one on the use of the BPaL regimen (i.e. bedaquiline, pretomanid and linezolid).
Who guidelines on tuberculosis infection prevention and control?
Wear a respirator around a family member with TB.
- Open windows to ventilate the room she is in.
- Sleep in a separate room to reduce the amount of time you spend breathing the same air.
- Stay home from work or school.
Who launches guidelines on management of latent TB?
Infection prevention and control consists of evidence-based measures intended to prevent exposure and reduce the risk of transmission of infectious agents. The revised guidelines contain recommendations for specific administrative, environmental controls and respiratory protection, following the assessment made by an external group of experts convened as members of the Guideline Development Group.
What is the WHO recommended treatment protocol for TB?
The preferred regimen for treating adults with TB remains a regimen consisting of an intensive phase of 2 months of isoniazid (INH), rifampin (RIF), pyrazinamide (PZA), and ethambutol (EMB) followed by a continuation phase of 4 months of INH and RIF.
WHO guidelines TB prevention?
The World Health Organization has updated its guidelines on tuberculosis preventive treatment. Among the 18 recommendations, the group now conditionally recommends shorter regimens as alternative treatment options: 1 month of daily rifapentine and isoniazid, or 4 months of daily rifampicin.
WHO latent TB treatment guidelines?
Preferred RegimensThree Months of Weekly Isoniazid Plus Rifapentine. ... Four Months of Daily Rifampin. ... Three Months of Daily Isoniazid Plus Rifampin.
What is the standard treatment for TB?
The most common treatment for active TB is isoniazid INH in combination with three other drugs—rifampin, pyrazinamide and ethambutol. You may begin to feel better only a few weeks after starting to take the drugs but treating TB takes much longer than other bacterial infections.
When does TB treatment start?
Treatment of latent TB infection should start after excluding the possibility of TB disease. Groups Who Should be Given High Priority for Latent TB Infection Treatment include: People with a positive TB blood test (interferon-gamma release assay or IGRA).
What are the 3 types of tuberculosis?
Tuberculosis: TypesActive TB Disease. Active TB is an illness in which the TB bacteria are rapidly multiplying and invading different organs of the body. ... Miliary TB. Miliary TB is a rare form of active disease that occurs when TB bacteria find their way into the bloodstream. ... Latent TB Infection.
WHO latent TB guidelines 2020?
Key RecommendationsThe first of three preferred regimens is once-weekly isoniazid plus rifapentine, for 3 months. ... The second preferred regimen, daily rifampin for 4 months, is also strongly recommended, especially for HIV-negative persons, and has perhaps the lowest toxicity.More items...•
What is the preferred treatment for latent TB?
CDC and the National Tuberculosis Controllers Association (NTCA) preferentially recommend short-course, rifamycin-based, 3- or 4-month latent TB infection treatment regimens over 6- or 9-month isoniazid monotherapy. Short course regimens include: Three months of once-weekly isoniazid plus rifapentine (3HP)
What is the best treatment for latent TB?
Isoniazid and Rifapentine (INH-RPT) are medicines used together to treat LTBI. They kill the sleeping TB germs before they make you sick. It can take many months for the medicine to kill the TB germs because they are strong.
What are 3 drugs for TB?
Rifampin (RIF),Isoniazid (INH),Pyrazinamide (PZA), and.Ethambutol (EMB)
What is the first line drug for TB?
First-line agents for treatment of active TB consist of isoniazid, a rifamycin (rifampin or [less frequently] either rifapentine or rifabutin), pyrazinamide, and ethambutol; in addition, moxifloxacin is a first-line agent when administered in combination with isoniazid, rifapentine, and pyrazinamide [6].
What is the duration of TB treatment?
You'll be prescribed at least a 6-month course of a combination of antibiotics if you're diagnosed with active pulmonary TB, where your lungs are affected and you have symptoms. The usual treatment is: 2 antibiotics (isoniazid and rifampicin) for 6 months.
How long does it take to treat TB?
TB disease can be treated by taking several drugs for 6 to 9 months. There are 10 drugs currently approved by the U.S. Food and Drug Administration (FDA) for treating TB. Of the approved drugs, the first-line anti-TB agents that form the core of treatment regimens are: isoniazid (INH) rifampin (RIF)
What is it called when TB bacteria multiply?
When TB bacteria become active (multiplying in the body) and the immune system can’t stop the bacteria from growing, this is called TB disease. TB disease will make a person sick. People with TB disease may spread the bacteria to people with whom they spend many hours.
What is XDR TB?
Extensively drug-resistant TB (XDR TB) is a rare type of MDR TB that is resistant to isoniazid and rifampin, plus any fluoroquinolone and at least one of three injectable second-line drugs (i.e., amikacin, kanamycin, or capreomycin). Treating and curing drug-resistant TB is complicated.
Can TB be treated?
It is very important that people who have TB disease are treated, finish the medicine, and take the drugs exactly as prescribed. If they stop taking the drugs too soon, they can become sick again; if they do not take the drugs correctly, the TB bacteria that are still alive may become resistant to those drugs.
What are the WHO recommendations for preventing tuberculosis?
New WHO recommendations to prevent tuberculosis aim to save millions of lives. Geneva – New World Health Organization (WHO) guidance will help countries accelerate efforts to stop people with tuberculosis (TB) infection becoming sick with TB by giving them preventive treatment. A quarter of the world‘s population is estimated to be infected ...
What is preventive treatment for TB?
TB preventive treatment is an affordable intervention that can prevent families from sliding into poverty and preserve the health and economy of whole communities. WHO anticipates that as new and safer drugs come onto the markets, and as prices fall, it will become a highly-cost effective way to save millions of lives.
How many people died from TB in 2018?
In 2018, 10 million people fell ill with TB worldwide and 1.5 million people lost their lives to this disease. “COVID-19 is highlighting just how vulnerable people with lung diseases and weakened immune systems can be,“ said Dr Tedros Adhanom Ghebreyesus, WHO Director-General. “The world committed to end TB by 2030;
What test is used to test for TB?
WHO recommends that either a tuberculin skin test or interferon-gamma release assay (IGRA) be used to test for TB infection. Both tests are helpful to find people more likely to benefit from TB preventive treatment but should not become a barrier to scale-up access.
When is World TB Day?
World TB Day is observed on March 24 each year to raise public awareness and understanding about the world’s deadliest infectious killer – TB and its devastating health, social and economic impact on people around the world.
Is TB contagious?
A quarter of the world‘s population is estimated to be infected with TB bacteria. These people are neither sick nor contagious. However, they are at greater risk of developing TB disease, especially those with weakened immunity.
Is TB a cause of death?
TB remains the top cause of death among people with HIV. TB preventive treatment works synergistically with antiretroviral therapy to prevent TB and save lives. Reinvigorated efforts by governments, health services, partners, donors and civil society will be needed to increase access to TB preventive treatment to the levels targeted.
Module 1: Prevention
There are 18 recommendations in the 2020 update. The main changes include conditional recommendations for a 1 month daily rifapentine and isoniazid regimen, and a 4 month daily rifampicin regimen as alternative treatment options.
Module 3: Diagnosis
This document consolidates five guidelines developed by WHO between 2016 and 2020. A range of new diagnostic technologies have been endorsed by WHO between 2010 and 2020. This document provides background, justification and recommendations on these technologies.
Module 4: Treatment
This second module includes a comprehensive set of WHO recommendations for the treatment and care of people with drug resistant TB. The document includes two new recommendations. The first is on the composition of shorter regimens and the second is on the use of the BPaL regimen (i.e. bedaquiline, pretomanid and linezolid).
Social Media
If you have found this page useful please tell other people about TBFacts.org and if you have a website please link to us at https://tbfacts.org/who-tb-guidelines/.
What is the first line of anti-TB drugs?
Of the approved drugs, the first-line anti-TB agents that form the core of treatment regimens are: isoniazid (INH), rifampin (RIF), ethambutol (EMB), and. pyrazinamide (PZA). Regimens for treating TB disease have an intensive phase of 2 months, followed by a continuation phase of either 4 or 7 months. The continuation phase should be extended ...
When should sputum be collected for TB?
Sputum specimens for microscopic examination and culture should be obtained from patients diagnosed with TB disease at a minimum of monthly intervals until two consecutive specimens are negative on culture. It is critical to obtain a sputum specimen at the end of the intensive phase (2 months) to determine if the continuation phase should be extended. In addition, it is essential that patients have clinical evaluations at least monthly to identify possible adverse effects of the anti-TB medications and to assess adherence. All patients with TB disease should have counseling and testing for HIV.
What is a DOT in TB?
DOT is a strategy in which a health care worker or another designated person watches the TB patient swallow each dose of the anti-TB drugs. All patients taking drugs fewer than 7 days per week (e.g., 1, 2, 3, or 5 days a week) must receive DOT.
How is treatment completion determined?
Treatment completion is determined by the number of doses ingested over a given period of time. Although basic TB regimens are broadly applicable, there are modifications that should be made under special circumstances (i.e., HIV infection, drug resistance, pregnancy, or treatment of children).
Is TB a public health function?
Treating tuberculosis (TB) disease benefits not only the individual patient but the community as a whole.Thus, any health care provider undertaking treatment of a patient with TB, whether a public health or private practitioner, is assuming a public health function that includes the responsibility for not only prescribing an appropriate regimen but also ensuring the patient’s adherence to the regimen until treatment is completed.
Further reading
WHO consolidated guideline on drug-resistant tuberculosis treatment. (WHO/CDS/TB/2019.4). Geneva, World Health Organization, 2019
Acknowledgement
We would like to thank the colleagues from the Global Fund to Fight AIDS, Tuberculosis and Malaria, United States Agency for International Development and the Global Drug Facility of the Stop TB Partnership for their comments and contribution to the FAQs.
How long do you have to take antibiotics for tuberculosis?
For active tuberculosis, you must take antibiotics for at least six to nine months. The exact drugs and length of treatment depend on your age, overall health, possible drug resistance and where the infection is in your body.
What is the test for TB?
Sputum tests. If your chest X-ray shows signs of tuberculosis, your doctor might take samples of your sputum — the mucus that comes up when you cough. The samples are tested for TB bacteria. Sputum samples can also be used to test for drug-resistant strains of TB.
How long does ethambutol last?
If you have drug-resistant TB, a combination of antibiotics called fluoroquinolones and injectable medications, such as amikacin or capreomycin (Capastat), are generally used for 20 to 30 months. Some types of TB are developing resistance to these medications as well.
What test is used to test for tuberculosis?
The most commonly used diagnostic tool for tuberculosis is a skin test, though blood tests are becoming more commonplace. A small amount of a substance called tuberculin is injected just ...
Can a TB test be wrong?
Results can be wrong. The TB skin test isn't perfect. Sometimes, it suggests that people have TB when they don't. It can also indicate that people don't have TB when they do. You can have a false-positive result if you've been vaccinated recently with the bacille Calmette-Guerin (BCG) vaccine.
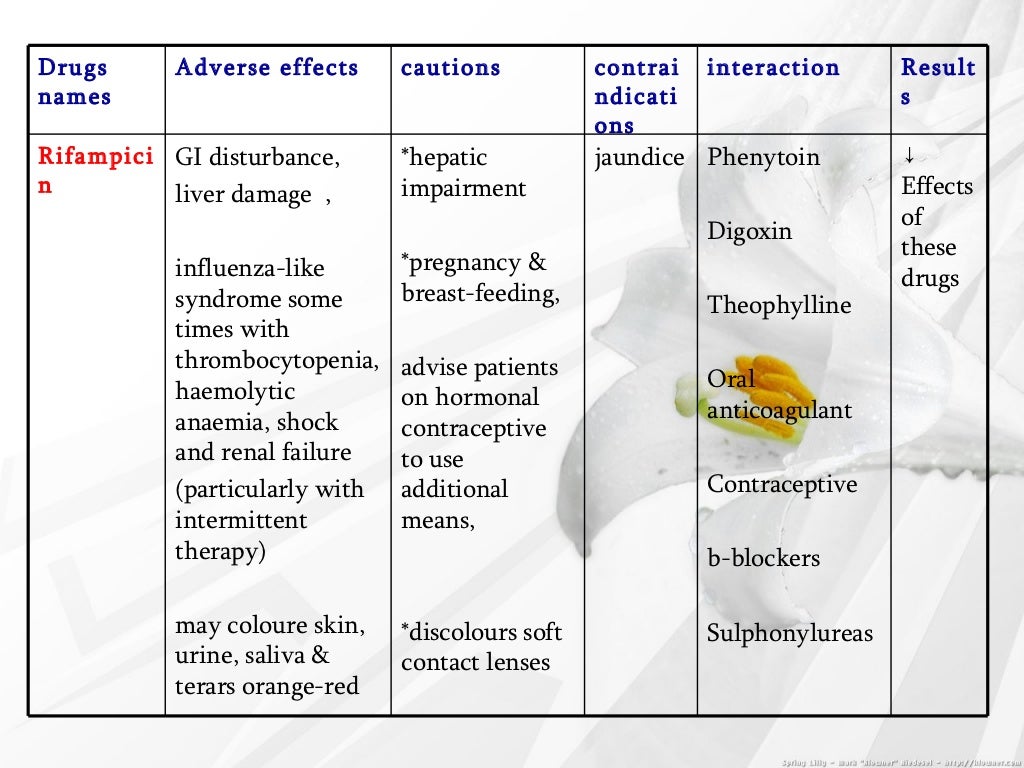
Can TB drugs cause liver damage?
Serious side effects of TB drugs aren't common but can be dangerous when they do occur. All tuberculosis medications can be toxic to your liver. When taking these medications, call your doctor immediately if you have any of the following:
What should a clinic decide on TB treatment?
Clinicians should choose the appropriate treatment regimen based on drug susceptibility results of the presumed source case (if known), coexisting medical conditions (e.g., HIV. ), and potential for drug-drug interactions. Consultation with a TB expert is advised if the known source of TB infection has drug-resistant TB.
What is the name of the drug that is used to treat TB?
Isoniazid (INH) Rifapentine (RPT) Rifampin (RIF) These medications are used on their own or in combination, as shown in the table below. CDC and the National Tuberculosis Controllers Association (NTCA) preferentially recommend short-course, rifamycin-based, 3- or 4-month latent TB infection treatment regimens over 6- or 9-month isoniazid ...
Is 6H or 9H better for TB?
Although effective, 6H and 9H have higher toxicity risk and lower treatment completion rates than most short-term treatment regimens. All treatment must be modified if the patient is a contact of an individual with drug-resistant TB disease.
How long does it take to treat TB in children?
Children over 2 years of age can be treated for latent TB infection with once-weekly isoniazid-rifapentine for 12 weeks. Alternative treatments for latent TB infection in children include 4 months of daily rifampin or 9 months of daily isoniazid.
Why is treatment recommended for children with latent TB?
Treatment is recommended for children with latent TB infection to prevent them from developing TB disease. Infants, young children, and immunocompromised children with latent TB infection or children in close contact with someone with infectious TB disease, require special consideration because they are at increased risk for getting TB disease.
How long does it take for TB to go away?
TB disease is treated by taking several anti-TB medicines for 6 to 9 months. It is important to note that if a child stops taking the drugs before completion, the child can become sick again. If drugs are not taken correctly, the bacteria that are still alive may become resistant to those drugs.
Why is TB so common in adults?
In comparison to children, TB disease in adults is usually due to past TB infection that becomes active years later, when a person’s immune system becomes weak for some reason (e.g., HIV infection, diabetes).
Can children take TB medicine?
It is very important that children or anyone being treated for latent TB infection or TB disease take the drugs exactly as instructed by the doctor and finish the medicine.
When should antiretroviral therapy be initiated?
Anti-retroviral therapy should ideally be initiated within the first 2 weeks ...
How long does HIV treatment last?
In the uncommon situation in which HIV-infected patients do NOT receive antiretroviral therapy during TB treatment, prolonging treatment to 9 months (extend continuation phase to 7 months) is recommended. Prolonging treatment to 9 months (extend continuation phase to 7 months) for HIV-infected patients with delayed response to therapy (e.g., ...
What is DOT therapy?
Directly observed therapy (DOT) and other adherence promoting strategies should be used in all patients with HIV-related TB. The care for HIV-related TB should be provided by, or in consultation with, experts in management of both TB and HIV. The care for persons with HIV-related TB should include close attention to adherence to both regimens of TB and antiretroviral treatment, drug-drug interactions, paradoxical reaction or Immune Reconstitution Inflammatory Syndrome (IRIS), side effects for all drugs used, and the possibility of TB treatment failure or relapse.
Is latent TB more likely to develop HIV?
Latent TB Infection and HIV. Someone with untreated latent TB infection and HIV infection is much more likely to develop TB disease during his or her lifetime than someone without HIV infection. There are several effective latent TB treatment regimens available for people with HIV.
Can you take rifabutin with HIV?
Four months of daily rifampin is another treatment option. This regimen should not be used in people with HIV who are taking some combinations of antiretroviral therapy. In situations where rifampin cannot be used, sometimes another drug, rifabutin , may be substituted. For those taking antiretroviral medications with clinically significant drug ...
Introduction
Recommended Regimens
- There are 10 drugs currently approved by the U.S. Food and Drug Administration (FDA) for treating TB. Of the approved drugs, the first-line anti-TB agents that form the core of treatment regimens are: 1. isoniazid (INH), 2. rifampin (RIF), 3. ethambutol (EMB), and 4. pyrazinamide (PZA). Regimens for treating TB disease have an intensive phase of 2 ...
Hiv-Negative Persons
- A continuation phase of once-weekly INH and rifapentine can be used for HIV-negative patients who do not have cavities on the chest film and who have negative acid-fast bacilli (AFB) smears at the completion of the intensive phase of treatment.
Case Management
- Patient-centered case management should be used in the treatment strategy with an adherence plan that includes directly observed therapy (DOT). DOT is a strategy in which a health care worker or another designated person watches the TB patient swallow each dose of the anti-TB drugs. All patients taking drugs fewer than 7 days per week (e.g., 1, 2, 3, or 5 days a week) mustreceive DOT.
Follow-Up Evaluations
- Sputum specimens for microscopic examination and culture should be obtained from patients diagnosed with TB disease at a minimum of monthly intervals until two consecutive specimens are negative on culture. It is critical to obtain a sputum specimen at the end of the intensive phase (2 months) to determine if the continuation phase should be extended. In addition, it is essential …
For More Information
- Official American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis. Clin I...
- Special Considerations for Treatment of TB Disease in Persons Infected with HIV (Fact Sheet). Available online at https://www.cdc.gov/tb/publications/factsheets/treatment.htm