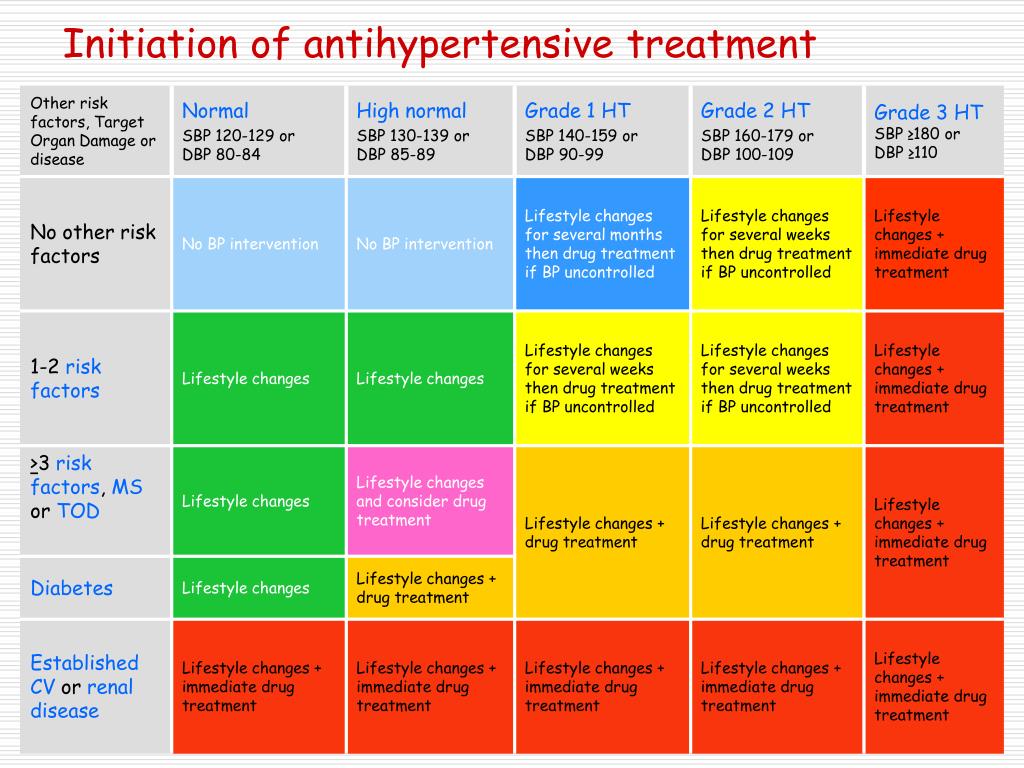
When should antihypertensive drug treatment be initiated in patients with hypertension?
The first recommendation is that of initiating antihypertensive drug treatment when systolic blood pressure is at least 140 or diastolic blood pressure at least 90 mmHg in patients with grade 1 hype … The evidence for two recommendations of all major guidelines on hypertension is critically discussed.
How do I take antihypertensive drugs?
Most people take antihypertensive drugs in the form of a pill you swallow every day, but your provider can give you some antihypertensive medications through an IV in your arm during a hospital stay. Cleveland Clinic is a non-profit academic medical center.
When to start antihypertensive therapy after a stroke or TIA?
Those not previously treated for hypertension and who have a BP ≥140/90 mm Hg should begin antihypertensive therapy a few days after the index event. Selection of drugs should be based on comorbidities. A goal of <130/80 mm Hg may be reasonable for those with a stroke or TIA.
Can you start and stop antihypertensive drugs without results?
They may also start and stop antihypertensive drugs if they aren’t giving results. Most people take antihypertensive drugs in the form of a pill you swallow every day, but your provider can give you some antihypertensive medications through an IV in your arm during a hospital stay.
What is the target BP for kidney disease?
In patients with chronic kidney disease, the target BP is 130/80. For patients with type 2 diabetes mellitus (T2DM), it is recommended to start on antihypertensive medications if BP is more than 130/80 with a goal of BP lower than 130/80.
What is the HTN stage?
The 2017 American College of Cardiology (ACC) and American Heart Association (AHA) definition of HTN stages is: Normal blood pressure (BP): systolic BP is less than 120, and diastolic BP is less than 80. Elevated BP: systolic BP 120 to 130 ...
How do beta blockers work?
Beta-blockers work by inhibiting the catecholamines from binding to the Beta 1,2, and 3 receptors. Beta-1 receptors are found primarily in the heart muscle, beta-2 receptors are located in the bronchial and peripheral vascular smooth muscles, and beta-3 receptors appear in adipose tissue of the heart.
Does hydrochlorothiazide lower blood pressure?
Switching to chlorthalidone from hydrochlorothiazide decreases systolic blood pressure by 7 to 8 mm Hg.
Is spironolactone a good antihypertensive?
Spironolactone is superior to doxazosin and bisoprolol in lowering blood pressure when added to first-line antihypertensive agents in treating resistant hypertension. [28] Hydralazine can be added for the treatment of resistant hypertension, either alone or in combination with nitrates, in case of heart failure.
Is a beta blocker a diuretic?
The beta-blocker and diuretic combination is associated with a higher incidence of diabetes. Clinicians should use combinations containing beta-blockers when beta-blockers are indicated in patients with heart failure, tachycardia, or post-MI patients.
Can you take two antihypertensive medications at once?
A combination of two antihypertensive medications should be a therapeutic option for patients with stage 2 hypertension .[6] . One study showed a reduction in blood pressure when drugs from two different classes are combined is approximately five times greater than when the dose of one drug dose doubles. [18]
Tailoring Antihypertensive Treatment
In the early 1970s, Laragh’s group coined the terms low-renin, normal-renin, and high-renin hypertension by relating plasma renin activity to the daily sodium excretion. 21 Under normal conditions, plasma renin activity increases with sodium restriction but decreases with higher BP.
Control Rates on Monotherapy Versus Combination Therapy
With as objective to estimate the proportion of patients with hypertension who can be controlled on monotherapy, we reviewed the placebo-controlled randomized clinical trials listed in systematic reviews of BP-lowering therapies 13–17 as well as the trials of intensive versus usual BP control.
Evidence Supporting SPCs
The literature on SPCs focuses on efficiency, adherence (also known as compliance), 44 persistence, and safety. Over time, these notions permeated to several, 1–9 but not all, 10–12 guidelines. What is the evidence?
Take Home Messages
Table 2 lists the major limitations of the recommended policy to initiate antihypertensive treatment using SPCs in most patients. 1, 2
Acknowledgment
We acknowledge the clerical assistance of Vera De Leebeeck and Renilde Wolfs, Research Unit Hypertension and Cardiovascular Epidemiology, Department of Cardiovascular Sciences, University of Leuven, Leuven, Belgium.
Source of Funding
The Research Institute Alliance for the Promotion of Preventive Medicine received a nonbinding grant from OMRON Healthcare Co Ltd, Kyoto, Japan.
Footnotes
The opinions expressed in this article are not necessarily those of the editors or of the American Heart Association.
What is the risk of stage 2 hypertension?
For those with stage 2 hypertension or with preexisting cardiovascular disease, diabetes mellitus, chronic kidney disease, or a 10-year risk of cardiovascular disease of 10% or higher , both lifestyle change and medication are recommended.
Can blood pressure medications reduce blood pressure?
A: Multiple clinical trials have shown that blood pressure can be effectively reduced by medications and that doing so results in a reduced incidence of target-organ events. The initial agent can be selected from one of four drug classes: angiotensin-converting–enzyme (ACE) inhibitors, angiotensin-receptor blockers (ARBs), calcium-channel blockers, and thiazide-type diuretics; each class has been shown to reduce cardiovascular events. The patient’s lifestyle, coexisting conditions, and clinical characteristics should be considered in selecting an agent. For example, patients with a high salt intake (e.g., eating primarily processed foods) may have a greater blood-pressure reduction with diuretic therapy, whereas those restricting salt intake may have a greater response to blockade of the renin–angiotensin system.
What is initial dual therapy?
However, in contrast with the 2013 guidelines, 2 in the 2018 guidelines, 1 initial dual therapy is the object of a strong recommendation rather than an advice and applies to a wider spectrum of hypertensive patients , thus becoming the standard approach.
Is SPC a first line therapy?
In this perspective, although the use of first-line SPC is considered as optimal in most hypertensive patients, the essential is to use dual therapy, even as combination of free drugs if SPCs are unavailable or unaffordable (see higher).
Is dual therapy effective for hypertension?
In conclusion, the use of dual therapy as first-line antihypertensive treatment in most hypertensive patients, preferably in the form of SPCs, appears as a pragmatic and effective means to improve BP control and thus decrease the associated cardiovascular burden worldwide.
Overview
Antihypertensives are medicines that bring your blood pressure down in various ways. Some antihypertensives make your blood vessels widen so blood gets through more easily. Others remove extra fluids from your blood or slow down your heartbeat.
Recovery and Outlook
Many people are successful in controlling their blood pressure with antihypertensive drugs. This helps prevent serious cardiovascular and kidney problems. People who keep their blood pressure in a normal range keep taking their medicine at the same time every day without missing doses.
When to Call the Doctor
Tell your provider if you’re having problems with antihypertensive side effects. They can order a different antihypertensive medication or give you a different amount (dose) of what you’re taking. Also, if your blood pressure readings get too high or too low on your home blood pressure monitor, tell your provider.
Frequently Asked Questions
You can take methyldopa, labetalol or nifedipine during pregnancy, but check with your provider for their recommendation. Many other antihypertensives are not safe for a developing fetus, so be sure to let your provider know when you plan to become pregnant.