What are the treatment options for benign lytic lesions of the femur?
Surgical treatment options for benign lytic lesions of the proximal femur include curettage, and bone grafting of the resulting defect with or without internal fixation. Most of these studies recommended either autogenous or allogenic bone graft. Local adjuvants may be used to control local recurrence of the aggressive lesions [1, 2, 4–8].
How to treat lytic lesions of bone?
Treatment Of Lytic Bone Lesions. It is necessary to prevent further deterioration of bone, alleviate pain and prevent fractures. In majority of cases medications are given to reduce the incidence of osteoporosis. Modern medicines are now available especially in case of cancer causing lytic lesions of bone.
What are the treatment options for osteolytic lesions of the hip?
Treatment of osteolytic lesions usually involves medications that control further loss of bone tissue and radiation therapy to alleviate pain and other accompanying symptoms.
What are lytic lesions of the bone marrow?
Also known as bone lesions or osteolytic lesions, lytic lesions are spots of bone damage that result from cancerous plasma cells building up in your bone marrow. Your bones can't break down and regrow (your doctor may call this remodel) as they should.
How are lytic bone lesions treated?
Typically, the most effective treatment for lytic lesions involves treatment of the underlying condition and supportive treatment for the bone. For example, common treatments for multiple myeloma may include : Chemotherapy: This treatment involves the use of certain drugs to kill rapidly dividing cancer cells.
What percentage of lytic lesions are cancerous?
Benign tumors and tumor-like lesions constitute about 79.3% of cases of all musculoskeletal lesions and show a slight female predominance. However malignant tumors constitute only 20.7% of lesions and show a male predominance.
Do lytic lesions mean cancer?
Also known as bone lesions or osteolytic lesions, lytic lesions are spots of bone damage that result from cancerous plasma cells building up in your bone marrow. Your bones can't break down and regrow (your doctor may call this remodel) as they should.
Are lytic bone lesions painful?
What Are Lytic Lesions? Lytic lesions are areas where bone has been destroyed, leaving a hole in the bone. These lesions in the spine are common, and when severe, can lead to one or more vertebral compression fractures, which can be painful and even disabling.
What is the treatment for bone lesions?
Malignant lesions always require treatment. Malignant lesions are usually treated with surgery to remove the tumor, but they may also require other forms of treatment, such as chemotherapy or radiation therapy.
Can you biopsy a lytic lesion?
We conclude that ultrasonically guided fine-needle aspiration biopsy is a useful technique to obtain a pathological diagnosis in cases of lytic bone lesions that can be visualized with this imaging technique.
What does a lesion on the femur mean?
Bone lesions are areas of bone that are changed or damaged. Causes of bone lesions include infections, fractures, or tumors. When cells within the bone start to divide uncontrollably, they are sometimes called bone tumors. Most bone lesions are benign, meaning they are not cancerous.
Where does myeloma spread to first?
At first, the cells reproduce in the bone marrow of the spine. From there, they enter the bloodstream and travel to bone marrow in other parts of the body. They collect in the bone marrow and the hard, outer part of the bones. As this progression happens, the plasma cells can cause multiple tumors.
Do lytic lesions show up on bone scan?
Bone scans generally are not sensitive for lytic bone lesions, and patients who show multiple myeloma or lytic abnormalities on computed tomography (CT) or x-ray should not be referred for a bone scan.
Which cancers cause lytic bone lesions?
There is a long list of lytic metastases but most primaries from the following common primary cancers are predominantly lytic 7: renal cancer. lung cancer. thyroid cancer.
Can bone lesions be repaired?
Current treatments which prevent bone further destruction cannot rebuild bone, therefore lesions are not repaired and fractures still occur.
What is life expectancy with multiple myeloma?
Multiple myeloma is an uncommon cancer of the blood. The median length of survival after diagnosis with multiple myeloma is 62 months for Stage I, 44 months for Stage II, and 29 months for Stage III. Life expectancy depends on many factors, including the person's age, health, kidney function, and more.
What causes femoral fractures?
... Pathological femoral fractures can result from various underlying diseases, such as infection, metabolic bone diseases, or bone tumors. Among bone tumors, metastatic disease is the most frequent malignant neoplasm of the bone, ranging from 25-85%, and usually originating from the prostate, breast, lung, kidney, or thyroid [5] [6] [7] [8]. The femur is the second most common metastasis site following the vertebra [9,10], with high susceptibility of progression to pathological fractures because the femur is a long, high load-bearing bone [11,12]. ...
What is intramedullary nailing?
Background: Antegrade intramedullary nailing is indicated for treating metastatic pathological femoral shaft fractures. Although good functional outcomes could be obtained from internal fixation, postoperative adverse events have been reported in patients with pathological fractures and non-pathological fractures. Not only adverse events but also their consequences including, readmission and reoperation, need to be considered. Few studies have assessed the risk of postoperative adverse events, reoperation, and readmission without comparison. Therefore, this study aimed to compare the risk of in-hospital adverse events and consequences after discharge between patients with metastatic pathological and non-pathological femoral fractures undergoing intramedullary nailing. Methods: We conducted a retrospective study by extracting records from the Hospital Information System database. We accessed patients with pathological metastatic pathological and non-pathological femoral shaft fractures undergoing intramedullary nailing by the International Classification of Diseases code; from June 2006 to 2020. We then tracked the in-hospital medical and surgical adverse events postoperatively, along with the consequences after discharge. The in-hospital adverse events risk between the two groups of patients were analyzed and compared by multivariate logistic regression analysis. Results: Included patients consisted of 48 in pathological groups and 185 in non-pathological groups. Significantly higher rates of surgical and medical adverse events in patients with pathological fractures compared to patients with non-pathological fractures were observed. After adjusting for potential confounding factors in multivariate regression analysis, patients with pathological fractures had higher odds of both adverse surgical (adjusted OR 2.43, 95% CI 1.15 - 5.13) and medical adverse events (adjusted OR 2.81, 95% CI 1.13 - 7.03). Conclusions: Patients with metastatic pathological femoral shaft fractures undergoing intramedullary nailing were more likely to experience postoperative adverse events than patients with non-pathological fractures.
What are the most common long bone defects in cancer patients?
Objectives: The femur is the most common long bone affected by cancerous metastasis. Femoral tumor defects are known to induce pain and functional impairment in patients. Although prior studies exist evaluating the clinical and biomechanical effect of tumor defect size, no biomechanical studies have experimentally examined the risk of pathological fracture with respect to the anterior, posterior, medial, and lateral surfaces on which a proximal tumor defect is located on the femur . Methods: Circular tumor-like defects of 40-mm diameter were created proximally in the subtrochanteric region on the Anterior (n = 5), Posterior (n = 5), Medial (n = 5), and Lateral (n = 5) sides of 20 synthetic femurs. Intact femurs served as a control group (n = 4). Femurs were tested for lateral, "offset" torsional, and axial stiffness, as well as axial strength. Results: Lateral stiffnesses (range, 121-162 N/mm) yielded no differences between groups (P = 0.069). "Offset" torsional stiffnesses (range, 135-188 N/mm) demonstrated that the Medial group was less stiff than the Intact, Anterior, and Lateral groups (P ≤ 0.012). Axial stiffnesses (range, 1057-1993 N/mm) showed that the Medial group was less stiff than the Intact group (P = 0.006). Axial strengths (range, 3250-6590 N) for the Medial group were lower than Anterior (P = 0.001) and Posterior (P = 0.001) specimens, whereas the Lateral group had a lower strength than Anterior specimens (P = 0.019). No other statistical differences were noted. Axial failure of Medial and Lateral specimens involved the tumor-like defect in 100% of cases, whereas 100% of Intact femurs and 80% of Anterior and Posterior femur groups failed only through the neck. Conclusions: In 2 of 3 test modes, the Medial tumor-like defect group resulted in statistically lower stiffness values compared with Intact femurs and had lower strength than Anterior and Posterior groups in axial failure.
Can proximal femoral metastases cause fracture?
Proximal femoral metastases can lead to pathologic fracture. The goals of this study were to improve guidelines for assessing pathologic hip fracture risk by quantifying the effect of location of femoral neck metastases on hip strength under single-limb stance loading and to evaluate the effectiveness of a proposed minimally invasive surgical repair technique for restoring hip strength. Twelve matched pairs of human cadaveric proximal femora were used to create a total of 564 finite element models before and after introduction and repair of simulated lytic defects, modeled as spherical voids, at various locations within the femoral neck. Defect site greatly affected hip strength (p < 0.001). Defects in the inferomedial aspect of the neck and in the dense trabecular bone near the base of the femoral head had the greatest effect, with hip strengths 23% to 72% and 43% to 64% that of the intact strength, respectively, for 20-mm diameter defects. Even so, the proposed percutaneous repair technique restored static strength of femora with defects at all of the studied locations. These findings may lead to a reduction in the number of patients who suffer a preventable pathologic fracture, a decreased likelihood of unnecessary surgery, and a less invasive prophylactic surgical procedure.
Abstract
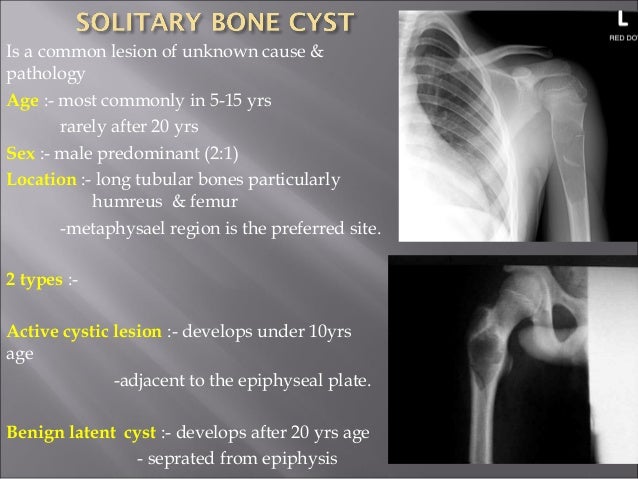
Thirty-five patients with a benign lesion of the femoral neck or trochanter were treated and seen in followup at the authors' institution from 1988 to 1991. Sixteen men and 19 women between the ages of 18 and 54 years (average, 27 years) were seen at an average followup of 3 years 6 months (range, 2-5 years).
MATERIALS AND METHODS
Seventy-three patients with benign bone lesions of the femoral neck and trochanter were surgically treated at the authors' institution from 1988 to 1991. Small lesions that can be treated with simple bone grafting, pinning, or palliative methods were excluded from this series.
RESULTS
Of the 35 patients, 16 were women and 19 were men. The average age of the patients was 27 years (range, 18-54 years). The pathologic diagnoses were 8 aneurysmal bone cysts (Fig 2); 14 monostotic fibrous dysplasias (Fig 3); 11 simple bone cysts (Fig 4); and 2 giant cell tumors.
DISCUSSION
The upper third of the femur is 1 of the most common sites of benign tumor involvement. The specific anatomic location makes the management of these lesions unique. Most of the lesions are small and silent. They need close observation or palliative treatment, especially in children.
Why do we need to treat lytic lesions?
Lytic lesions of bone need to be treated. It is necessary to prevent further deterioration of bone, alleviate pain and prevent fractures. In majority of cases medications are given to reduce the incidence of osteoporosis. Modern medicines are now available especially in case of cancer causing lytic lesions of bone.
What is a lytic bone lesion?
Lytic bone lesion is a general term used when the bone becomes extremely weak by a disease. Normal bone tissue constantly gets remodeling and repaired from time to time. Lytic lesion of bone is an area where the bone appears to have been eaten away. There are several diseases that can cause destruction of bone area.
What is osteolytic lesions?
Osteolytic lesions occur when there are structural changes in the process of bone formation and degradation. Normally the bone gets remodeling from time to time. The old cells of bone skeleton are destroyed and they are replaced by the new growth of bone cells.
What causes osteolysis in the bone?
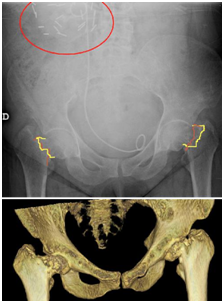
Aside from myeloma, there are several other conditions especially malignancies that may cause osteolysis. For example metastatic tumor from breast cancer, prostate, lung and thyroid cancer all can cause osteolytic lesion of bone. In majority of cases the lesions are found on skull, spine, long bone of leg, ribs, and pelvic bone.
Where are lesions found in the body?
In majority of cases the lesions are found on skull, spine, long bone of leg, ribs, and pelvic bone. Infection of bone can also lead to destruction and lysis of bone.
Does myeloma cause a hole in the bone?
This leads to formation of hole or moth eaten pattern in the bone structure due to destruction of more bone cells than its formation.
What is a lytic lesions?
Also known as bone lesions or osteolytic lesions, lytic lesions are spots of bone damage that result from cancerous plasma cells building up in your bone marrow. Your bones can't break down and regrow (your doctor may call this remodel) as they should.
What pain relievers are available for multiple myeloma?
Drugs that treat multiple myeloma pain include: Over-the-counter pain relievers, like acetaminophen, aspirin, ibuprofen, and naproxen.
What is the best medicine for multiple myeloma?
Opioids. These are stronger pain-fighting medicines that you get with a doctor's prescription. Morphine is one of the most common for multiple myeloma pain. Other opioids include codeine, fentanyl, hydrocodone, hydromorphone, methadone, and oxycodone. These come in pills, patches, lozenges, sprays.
What medications can help with multiple myeloma?
Some of these drugs, such as amitriptyline, duloxetine, and nortriptyline, can help treat nerve pain, called neuropathy, that often comes with multiple myeloma. Anticonvulsants. Medications like gabapentin ( Neurontin ), pregabalin ( Lyrica ), and topiramate (Topamax) also treat nerve pain. Corticosteroids.
What is the best treatment for numbness in the skin?
Anesthetics. Lidocaine skin patches, ointments, and gels can numb pain in specific areas. Your doctor can also inject anesthetic or anti-inflammatory drugs near a painful spot or nerve center, which is called a nerve block. Radiation.
