When should CLL be treated?
When to Treat CLL/SLL. To determine if treatment is needed, patients should talk with their providers about symptoms they are experiencing, swollen lymph nodes, and blood cell counts, according to Dr. Locke J. Bryan, associate professor of medicine at the Medical College of Georgia and the hematology/oncology fellowship program director at the Georgia Cancer Center at Augusta University.
How do you die from CLL?
Patients with leukemia may ultimately die due to multiple infections (bacteria, fungal, and/or viral), severe nutritional deficiencies, and failure of multiple organ systems. The patients can also face complications due to the leukemia treatment itself, which can sometimes be life-threatening. Some patients can go into complete remission.
How to cure CLL?
Until then, try to:
- Find out enough about your cancer to make decisions about your care. ...
- Turn to family and friends for support. Stay connected to family and friends for support. ...
- Connect with other cancer survivors. Consider joining a support group, either in your community or on the internet. ...
- Explore ways to cope with the nagging, chronic nature of the disease. ...
When do you treat CLL?
When treatment is needed, the main treatments used are: It's important to take time and think about your choices. Because CLL often grows slowly, not everyone needs to be treated right away. In choosing a treatment plan, the stage of the leukemia and other prognostic factors are important.

Can CLL SLL be cured?
There is no cure for either SLL or CLL. However, treatment can help improve a person's quality of life and slow the progression of the cancer. The cancer slowly progresses over the course of several years.
What is the best treatment for chronic lymphocytic leukemia?
Many different drugs and drug combinations can be used as the first treatment for CLL. The options include monoclonal antibodies, other targeted drugs, chemotherapy, and different combinations of these. Some of the more commonly used drug treatments include: Ibrutinib (Imbruvica), alone or with rituximab (Rituxan)
Are CLL and SLL treated the same?
CLL and SLL are slow-growing (low-grade or 'indolent') cancers. Many doctors group them together as a type of non-Hodgkin lymphoma. They usually behave like a long-term (chronic) condition that needs treatment from time-to-time to keep it under control. CLL and SLL are treated in the same way.
What is the difference between CLL and SLL leukemia?
CLL (chronic lymphocytic leukemia) and SLL (small lymphocytic lymphoma) are the same disease, but in CLL cancer cells are found mostly in the blood and bone marrow. In SLL cancer cells are found mostly in the lymph nodes. CLL/SLL is a type of non-Hodgkin lymphoma.
What is first line treatment for CLL?
Chemoimmunotherapy (CIT) has been the standard first-line therapy for CLL. Age and comorbidities can help decide which patients may benefit from a CIT approach. FCR (fludarabine, cyclophosphamide, and rituximab) is the current standard treatment option for younger patients with CLL.
How do you know if CLL is getting worse?
Unexplained weight loss of more than 10 percent of your body weight over the course of 6 months or so could mean your CLL is progressing. This means that you're losing weight when you're not trying to diet.
Which is worse SLL or CLL?
In fact, CLL and SLL are really the same disease. Sometimes patients with SLL can develop a rising white blood cell count in the blood (or leukemia), and patients with CLL invariably have CLL cells also in the lymph nodes. In addition, most cases of SLL become CLL over time.
When should CLL SLL be treated?
Patients with low-risk CLL/SLL do not receive treatment, but are followed every 3 to 6 months and donate cells (through apheresis) or lymph nodes, or both, for research purposes. Patients with intermediate or high-risk CLL/SLL receive standard treatment with rituximab and fludarabine for six 28-day treatment cycles.
What is the survival rate for SLL?
Small Lymphocytic Lymphoma Survival Rates The five-year survival rate for SLL in the United States is 86.9 percent. This means that, for every 100 people diagnosed with SLL now, about 87 people are expected to be alive in five years. This survival rate also applies to people with CLL.
Where does SLL spread to?
If you have SLL, these lymphocytes build up and grow in your lymph nodes, which are small, oval glands spread throughout the body that filter harmful substances out of your body through the lymphatic system.
What happens with SLL?
SLL/CLL can inhibit the immune system and make fighting infections more difficult. It can also cause the immune system to attack itself which is known as autoimmunity. When this occurs, two life-threatening conditions may develop.
What causes CLL SLL?
The exact cause of chronic lymphocytic leukemia is not known. Multiple genetic mutations occur in the DNA of blood-producing cells. These mutations cause the blood cells to produce abnormal lymphocytes, which are not effective at fighting infection. Usually, an abnormal chromosome is present in a patient with CLL.
What is the first treatment for CLL?
Initial treatment of CLL. Many different drugs and drug combinations can be used as the first treatment for CLL. The options include monoclonal antibodies, other targeted drugs, chemotherapy, and different combinations of these. Some of the more commonly used drug treatments include: Other drugs or combinations of drugs may also be used.
What is the most serious type of CLL?
One of the most serious complications of CLL is a change (transformation) of the leukemia to a high-grade or aggressive type of non-Hodgkin lymphoma (NHL) called diffuse large B-cell lymphoma (DLBCL) or to Hodgkin lymphoma. This happens in 2% to 10% of CLL cases, and is known as Richter's transformation. Treatment is often the same as it would be ...
How long does it take for chemo to lower blood count?
Chemo may not lower the number of cells until a few days after the first dose, so before the chemo is given, some of the cells may need to be removed from the blood with a procedure called leukapheresis. This treatment lowers blood counts right away.
What is the rarest complication of CLL?
If this happens, treatment is likely to be similar to that used for patients with ALL. Acute myeloid leukemia (AML) is another rare complication in patients who have been treated for CLL.
What happens if the first line of treatment is not working?
If the initial treatment is no longer working or the disease comes back, another type of treatment often helps . If the initial response to the treatment lasted a long time (usually at least a few years), the same treatment might be used again. If the initial response wasn't long-lasting, using the same treatment isn't as likely to be helpful. The options will depend on what the first-line treatment was and how well it worked, as well as the person's overall health.
What is the best treatment for enlarged spleen?
Radiation or surgery. If the only problem is an enlarged spleen or swollen lymph nodes in one part of the body, localized treatment with low-dose radiation therapy may be used. Splenectomy (surgery to remove the spleen) is another option if the enlarged spleen is causing symptoms.
What is the FCR for Venetoclax?
Bendamustine and rituximab (or another monoclonal antibody) High-dose prednisone and rituximab. FCR: fludarabine, cyclophosphamide, and rituximab. PCR: pentostatin, cyclophosphamide, and rituximab. Chlorambucil and rituximab (or another monoclonal antibody) Obinutuzumab.
What is the symptom of CLL and SLL?
One symptom of CLL and SLL is swollen lymph nodes; the location of the swelling could play a role in whether or not the disease is treated. “It’s about location … a big node may not be causing any problems, but a smaller node pushing on an organ may cause some problems.
When was Venclexta approved?
Since then, there have been three more approvals in the space: Venclexta (venetoclax), which was approved in 2016 ; Copiktra (duvelisib), which was approved in 2018; and Calquence (acalabrutinib), which was approved in 2019.
Does CLL need immediate treatment?
Treatments for chronic lymphocytic leukemia (CLL) and small lymphocytic leukemia (SLL) have drastically improved in recent years, although patients may not need immediate treatment directly after being diagnosed.
What are the best medications for CLL?
Common drugs or drug combinations used as initial treatments for CLL/SLL include: 1 Acalabrutinib (Calquence) 2 BR (bendamustine [Treanda] and rituximab [Rituxan]) 3 CG (chlorambucil [Leukeran] and obinutuzumab [Gazyva]) 4 FCR (fludarabine [Fludara], cyclophosphamide [Cytoxan], and rituximab) 5 FR (fludarabine and rituximab) 6 Ibrutinib (Imbruvica) 7 Ibrutinib-Obinutuzumab (Imbruvica-Gazyva) 8 Ibrutinib-rituximab (Imbruvica-Rituxan) 9 Ofatumumab (Arzerra) and chlorambucil 10 PCR (pentostatin, cyclophosphamide, and rituximab) 11 Rituximab and chlorambucil 12 Rituximab and Hyaluronidase and Human (Rituxan Hycela) 13 Venetoclax (venclexta)
Do patients with high risk disease need to start treatment right away?
However, patients with high-risk disease may need to start treatment right away.
What is the best treatment for CLL?
One of the most promising future treatment options for CLL is CAR T-cell therapy. CAR T, which stands for chimeric antigen receptor T-cell therapy, uses a person’s own immune system cells to fight cancer.
How many clinical trials are there for CLL?
These new treatments may work better for you than the ones currently available. There are currently hundreds of clinical trials ongoing for CLL.
Why are targeted therapies called targeted therapies?
These drugs are called targeted therapies because they’re directed at specific proteins that help CLL cells grow. Examples of targeted drugs for CLL include:
What is CLL in medical terms?
Chronic lymphocytic leukemia (CLL) is a slow-growing cancer of the immune system. Because it’s slow-growing, many people with CLL won’t need to start treatment for many years after their diagnosis.
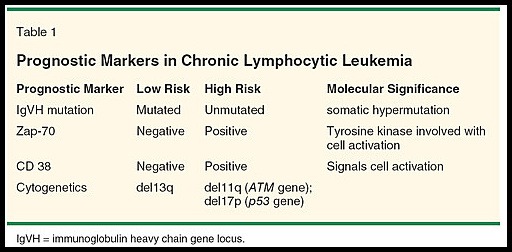
What does it mean when you have a high risk CLL?
High-risk CLL describes patients with stage 3 or stage 4 cancer. This means you may have an enlarged spleen, liver, or lymph nodes. Low red blood cell counts are also common. In the highest stage, platelet counts will be low as well.
What is intermediate risk CLL?
Intermediate-risk CLL describes people with stage 1 to stage 2 CLL, according to the Rai system. People with stage 1 or 2 CLL have enlarged lymph nodes and potentially an enlarged spleen and liver, but close to normal red blood cell and platelet counts. High-risk CLL describes patients with stage 3 or stage 4 cancer.
What is low risk CLL?
Treatments for low-risk CLL. Doctors typically stage CLL using a system called the Rai system. Low-risk CLL describes people who fall in “stage 0” under the Rai system. In stage 0, the lymph nodes, spleen, and liver aren’t enlarged. Red blood cell and platelet counts are also near normal. If you have low-risk CLL, ...
CLL: Bone marrow and blood cells
CLL also affects the immune system. However, in CLL, the cancer cells appear mainly in the bone marrow and blood cells. Bone marrow is the spongy tissue in the middle of the bones that makes substances that produce blood cells.
Cellular differences
When doctors examine the cancer cells under a microscope, both SLL and CLL look the same. However, there are some differences in the blood.
Physical exam
If a person does have symptoms, SLL diagnosis generally starts with a physical exam. During the exam, the doctor will ask the person about any symptoms they are having and review the person’s medical history. The doctor will also check for enlarged lymph nodes and signs of an enlarged spleen in the abdomen.
Blood tests
Based on what the doctor finds during the physical examination, they may then order blood tests. Blood tests that can help a doctor diagnose SLL include:
Bone marrow biopsy
While blood tests can determine whether or not a person has SLL, a doctor may still order a bone marrow aspiration and biopsy.
Additional tests
A doctor may order additional testing to help determine the best course of treatment. These tests can include:
What is the best treatment for chronic lymphocytic leukemia?
Here are some of the newest treatments for Chronic Lymphocytic Leukemia (CLL): Brukinsa (Zanubrutinib)2,3. Brukinsa (Zanubrutinib) is a kinase inhibitor indicated for the treatment of adult patients with mantle cell lymphoma ...
How does acute leukemia affect the cells?
In the event of acute leukemia, the immature blood cells increase rapidly, while in chronic leukemia the cells develop in a more normal manner, resulting in the disease taking longer to set in. 1.
What is Venclyxto chemo?
Venclyxto/Venclexta (venetoclax)7, Venclexta/Venclyxto (venetoclax) is a B-Cell lymphoma-2 (BCL-2) inhibitor (chemotherapy) indicated as monotherapy for the treatment of people with chronic lymphocytic leukemia (CLL), with or without the 17p deletion, who have received at least one prior therapy. Venclexta/Venclyxto (venetoclax) was approved by: ...
Can you treat CLL without 17p?
As monotherapy it is indicated for the treatment of patients with CLL with 17p deletion who have received at least one prior therapy, or patients with CLL without the 17p deletion who have received at least one prior therapy and for whom there are no other available treatment options.