Procedures
Likewise, people ask, what is the life expectancy of someone with aortic stenosis? Without treatment, the average life expectancy after the onset of heart failure due to aortic stenosis is between 6 to 24 months.
Self-care
According to research, patients with severe aortic valve stenosis who do not undergo any treatment can undergo sudden death in a span of two to three years. Surgery and medical treatment is seen to improve the life expectancy, increasing it up to 10 to 15 years of time after surgery.
Nutrition
When people do experience symptoms of aortic stenosis, they can include:
- Shortness of breath
- Dizziness or fainting
- Fatigue or reduced ability to do activities requiring mild exertion
- Chest pain, pressure or tightness
- Palpitations or a feeling of heavy, pounding, or noticeable heartbeats
What is the life expectancy of someone with aortic stenosis?
Patients with moderate aortic stenosis (AS) have an increased mortality compared with the general population, mainly related to associated comorbidities. Cardiovascular risk factors are frequent in patients with moderate AS and must be appropriately managed. The cumulative incidence of aortic valve replacement at 6 years is high, reaching 30%.
How long does someone with aortic stenosis live?
What is the prognosis with aortic valve replacement?
Is moderate aortic stenosis dangerous?
See more

What is the treatment of choice for aortic stenosis?
The only definitive treatment for aortic stenosis in adults is aortic valve replacement, performed surgically or percutaneously. The development of symptoms due to aortic stenosis provides a clear indication for replacement.
Can aortic stenosis be treated with medication?
Medications. No pill can cure or even improve your aortic stenosis.
How long can you live with mild aortic stenosis?
Without treatment, a person's life expectancy with aortic stenosis after symptoms develop is 1–3 years. Around 50–68% of symptomatic people die within 2 years. Often, they die suddenly. However, aortic valve replacement surgery significantly increases life expectancy.
What is the most common cause of aortic stenosis?
Aortic stenosis is most commonly caused by calcium buildup on the aortic valve over time. These calcium deposits that often come with age make the valve tissue stiff, narrow, and unyielding.
Can aortic stenosis be reversed without surgery?
However, there are no medications that can reverse aortic stenosis. The only cure is replacing the diseased valve. Usually, heart valve replacement requires open-heart surgery.
What worsens aortic stenosis?
Older age. Certain heart conditions present at birth (congenital heart disease) such as a bicuspid aortic valve. History of infections that can affect the heart. Having cardiovascular risk factors, such as diabetes, high cholesterol and high blood pressure.
At what point does aortic stenosis require surgery?
ANSWER: Whether you need surgery to replace your aortic valve due to aortic stenosis depends on the severity of your condition. Mild to moderate aortic stenosis typically does not require surgery. But, surgery is necessary for severe cases of aortic stenosis.
What are signs that aortic stenosis getting worse?
Call your doctor about new or worsening symptoms, including:Chest pain or tightness.Rapid fluttering heartbeat.Shortness of breath.Dizziness or faintness.Increased exhaustion after activity.Swollen ankles and feet.Difficulty sleeping.
How do you prevent aortic stenosis from getting worse?
To prevent this, brush your teeth twice each day and get regular cleanings. Let your dentist know that you have aortic stenosis. Don't put off surgery. Your doctor may advise surgery to repair or replace your damaged valve.
What happens if you don't treat aortic stenosis?
If left untreated, severe aortic stenosis can lead to heart failure. Intense fatigue, shortness of breath, and swelling of your ankles and feet are all signs of this. It can also lead to heart rhythm problems (arrhythmias) and even sudden cardiac death.
What medications should be avoided with aortic stenosis?
Antihypertensive treatment with β-blockers has generally been avoided in patients with severe aortic stenosis (AS) due to the concerns for inducing left ventricular dysfunction and hemodynamic compromise in the presence of severe outflow tract obstruction.
How quickly does aortic stenosis progress?
The present observations serve principally to indicate that progression does occur, that progression from noncritical to critical aortic stenosis can occur in less than five years, and that this is very likely to be found when patients with progressive symptoms and electrocardiographic changes are restudied.
How to diagnose aortic valve stenosis?
To diagnose aortic valve stenosis, your doctor will review your signs and symptoms, discuss your medical history, and do a physical examination. He or she will listen to your heart with a stethoscope to determine if you have a heart murmur that may signal an aortic valve condition.
What test is used to determine if you have aortic valve stenosis?
Tests also can help determine a cause and the condition's severity. Tests for aortic valve stenosis may include: Echocardiogram. This test uses sound waves to create images of your heart in motion.
What is the purpose of a aortic valve test?
Exercise tests help your doctor determine whether signs and symptoms of aortic valve disease occur during physical activity. These tests can help determine the severity of your condition. If you are unable to exercise, medications that have similar effects as exercise on your heart may be given to complete the test.
How is a replacement valve inserted?
A replacement valve is inserted through the catheter and guided to your heart. A balloon is expanded to press the valve into place. Some TAVR valves are self-expanding. You may eventually need surgery to repair or replace the diseased aortic valve, even if you don't have symptoms.
How to repair aortic valve?
Surgery to repair or replace an aortic valve is usually done through a cut (incision) in the chest. Less invasive approaches may be available. Ask your doctor if you're a candidate for these procedures. Aortic valve surgery may be done at the same time as other heart surgery.
What is a cardiac CT scan?
Cardiac computerized tomography (CT) scan. A cardiac CT scan combines several X-ray images to provide a more detailed cross-sectional view of the heart. Doctors may use cardiac CT to measure the size of your aorta and look at your aortic valve more closely. Cardiac MRI.
Can aortic valve surgery be done at the same time as heart surgery?
Aortic valve surgery may be done at the same time as other heart surgery. Surgery options for aortic valve stenosis include: Aortic valve repair. To repair an aortic valve, surgeons separate valve flaps (cusps) that have fused. However, surgeons rarely repair an aortic valve to treat aortic valve stenosis.
How long can a patient with aortic stenosis live without symptoms?
Patients with aortic stenosis can do well over many years without symptoms or limitations at rest or when active.
What is SAVR surgery?
During a surgical aortic valve replacement (SAVR), you would be put under general anesthesia, and you would be placed on a ventilator while on a heart-lung bypass machine. A surgeon would then cut open your breastbone (called a sternotomy) to get to the heart. In some patients, less invasive approaches can be used.
What is the procedure called when you have no symptoms?
Develop chest discomfort with activities. Lightheaded or even pass out. "Watchful observation" is recommended while patients have no symptoms. Once symptoms are present, replacing the valve may be considered. The less invasive procedure is also referred to as transcatheter aortic valve implantation, or TAVI.
Does a tavr valve need sternotomy?
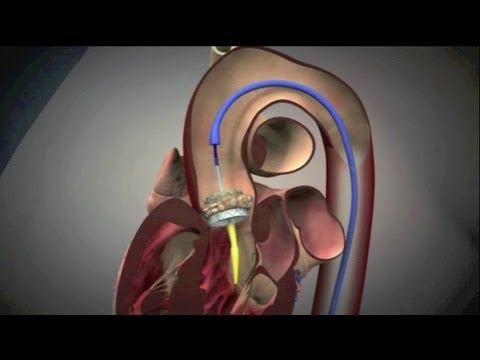
TAVR does not require sternotomy or a heart-lung bypass machine. The replacement valve is usually inserted using a catheter into an artery in the leg, then threaded through arteries to the heart. Once within the diseased aortic valve, the folded TAVR valve is opened with a balloon and the old valve pushed to the side.
Can a TAVR be replaced?
Surgery: The valve can be replaced either through surgery or using a less invasive procedure called transcatheter aortic valve replacement (TAVR). Both approaches reduce symptoms and help patients live longer. At present, no medical therapy can "unclog" an obstructed aortic valve.
Is a TAVR valve a major concern?
Overall, TAVR has been an exciting development in treating patients with aortic stenosis, but there are limitations: There is almost always a leak between the old and the new TAVR valve; however, this is usually not a major concern.
Does a TAVR valve last?
The TAVR valves may not last as long. It is important to talk with your heart doctor and heart surgeon to weigh the options for treatment of your aortic stenosis and decide what is right for you. Last Edited 12/17/2020. Medical Reviewer (s):
How to replace aortic valve?
Open Heart Surgery#N#(Also Known as Surgical Aortic Valve Replacement) 1 Typically during open heart surgery, the surgeon will make an incision across the full length of your chest to access your valve. 2 Sometimes open heart surgeries can be performed through smaller incisions (called minimal incision valve surgery#N#icon-zoom-in#N#). 3 Your old aortic valve will be taken out and a new one will be placed in your body. 4 The new valve can either be a mechanical valve#N#icon-zoom-in#N#or a bioprosthetic valve#N#icon-zoom-in#N#. 5 Talk to your doctor about questions you may have about open heart surgery and/or its associated risks.
What is BAV in aortic stenosis?
Your doctor may recommend balloon valvuloplasty (BAV) icon-zoom-in. to relieve symptoms of severe aortic stenosis. However, it is not a lasting solution as the valve will eventually narrow again.
What is Open Heart Surgery?
Explore how open heart surgery is performed and what you can expect from the procedure.
How does an open heart surgeon work?
Typically during open heart surgery, the surgeon will make an incision across the full length of your chest to access your valve. ). Your old aortic valve will be taken out and a new one will be placed in your body. . Talk to your doctor about questions you may have about open heart surgery and/or its associated risks.
Can you postpone aortic stenosis?
Postponing treatment for severe aortic stenosis could increase the risk of complications. Now’s not the time to wait. The sooner you treat severe aortic stenosis, the sooner you can get back to the life you want to live. to relieve symptoms of severe aortic stenosis.
Does TAVR shorten recovery time?
TAVR may shorten your recovery time so you can resume normal activities.
Can a valve be replaced in aortic stenosis?
But it is important to remember that eventually your valve will likely need to be replaced.
Open-heart surgery
In open heart surgery, the surgeon makes an incision in the middle of the chest to remove the damaged valve and place a new one. Because the heart must be stopped for this procedure, the patient is on a heart-lung bypass machine during the operation.
Minimally invasive valve replacement
As with open-heart surgery, the patient must be on a heart-lung bypass machine during a minimally invasive valve replacement. However, the surgeon is able to perform the procedure via a much smaller incision in the chest, using a tiny camera and slender tools to remove and replace the damaged valve.
Transcatheter aortic valve replacement (TAVR)
TAVR is an even less invasive procedure we can offer to some patients, based on their evaluation. Instead of making an incision in the chest, the surgeon threads a catheter through a blood vessel to reach the heart, then inserts a new valve inside the old one.
Balloon aortic valvuloplasty
This minimally invasive procedure aims to widen the narrowed valve rather than replace it. A catheter with a tiny deflated balloon at its tip is threaded through a blood vessel until it reaches the damaged valve. At that point, the balloon is inflated to expand the narrowed valve. The balloon is then deflated and the catheter is withdrawn.
Treatments we specialize in
This minimally invasive procedure makes it possible to replace a faulty aortic valve without the risks or long recovery of open-heart surgery.
What is the best treatment for aortic stenosis?
Untreated, severe, symptomatic aortic stenosis is associated with a dismal prognosis. The only treatment shown to improve survival is aortic valve replacement ; however, before symptoms occur, aortic stenosis is preceded by a silent, latent phase characterized by a slow progression at the molecular, cellular, and tissue levels. In theory, specific medical therapy should halt aortic stenosis progression, reduce its hemodynamic repercussions on left ventricular function and remodeling, and improve clinical outcomes. In the present report, we performed a systematic review of studies focusing on the medical treatment of patients with aortic stenosis. Lipid-lowering therapy, antihypertensive drugs, and anticalcific therapy have been the main drug classes studied in this setting and are reviewed in depth. A critical appraisal of the preclinical and clinical evidence is provided, and future research avenues are presented.
What receptors are expressed in the aortic valve?
Human aortic valves express prorenin, renin, ACE, and angiotensin II type 2 receptors. 28 Angiotensin II stimulates the expression of inflammatory cytokines in human smooth muscle cells and monocytes. 30 RAAS inhibition in AS attenuates the chemotactic effects of angiotensin II on monocytes in the valve leaflet tissue, 29 an important cellular component in the development of atherosclerosis and calcification. Angiotensin II and chymase (another enzyme involved in the synthesis of angiotensin II) 84 expression is upregulated in stenotic aortic valves, 89 and blockade of the RAAS prevents valve calcification and hemodynamic progression of AS both in experimental models of AS and in humans. 31, 83
Does statin help with atherosclerosis?
Similarities in the pathophysiology of atherosclerosis and AS have led the scientific community to believe that treatment that has been proven to be effective in atherosclerosis could also be effective in slowing the progression of AS. Statin drugs have been the most extensively studied medical treatment in AS. Experimental data have shown that statin therapy reduces osteoblast activity and cholesterol deposition in valve leaflets ( Figure 1 ). 33, 34 An association between statin use and a lower rate of aortic valve calcification or hemodynamic deterioration has been shown in most 35 – 40 but not all 35, 36, 41 – 43 observational studies. This association was also shown in rheumatic AS 44 and in patients with bioprosthetic aortic valves. 45 It is interesting to note that 1 prospective observational study showed that in patients with moderate AS (AVA, 1.0–1.5 cm 2 ), progression of AS was slower among those with hypercholesterolemia who were treated with rosuvastatin than among patients with normal LDL levels who were not treated with a statin. 43 These observations created enthusiasm in the scientific community and led to the initiation of multiple randomized trials evaluating lipid-lowering therapy in AS. Unfortunately, none of these trials were able to demonstrate reduced hemodynamic progression, reduced aortic valve calcification, or improved clinical outcomes despite successfully decreasing serum LDL concentrations ( Table 1 ). 12 – 15 Except for the SEAS trial (Simvastatin and Ezetimibe in Aortic Stenosis), 15 none of these trials were powered to detect significant clinical benefits. A recent study-level meta-analysis comprising 2344 patients reported no significant improvement in hemodynamic parameters, AVR rates, or cardiovascular death. 46 In addition, 1 small-scale, randomized trial failed to show benefit of rosuvastatin on hemodynamic progression in congenital AS (mean age: rosuvastatin, 33±9 years; placebo, 32±10 years). 16 As a consequence of these negative trials, both the American Heart Association/American College of Cardiology and the European Society of Cardiology guidelines do not recommend the use of statins specifically and solely for the treatment of AS. 9, 10
Does warfarin cause aortic calcification?
Warfarin is used to induce aortic valve calcification in experimental models of AS. 128 Warfarin inhibits vitamin K–dependent osteocalcin and matrix Gla protein, an inhibitor of vascular calcification. 129 – 131 Retrospective evidence has also linked the use of warfarin to increased aortic and mitral valve calcification in humans, 132 and observational data suggest that warfarin treatment may be an independent predictor of hemodynamic progression of AS. 99 Awaiting confirmatory trials, the use of direct oral anticoagulants may be preferable in patients with AS who require anticoagulation. The vitamin K–dependent matrix Gla protein is an inhibitor of arterial calcification, 133 and levels of its dephosphorylated and underphosphorylated forms are higher in patients with AS than in healthy control subjects. 130 In addition, higher levels of its dysfunctional forms are associated with more aortic calcification and worse survival in patients with AS and may be a potential treatment target in the future. 130, 131 Table 3 summarizes ongoing randomized trials related to the medical treatment of AS.
How severe is aortic valve stenosis?
Aortic valve stenosis ranges from mild to severe. Signs and symptoms generally occur when narrowing of the valve is severe. Some people with aortic valve stenosis may not have symptoms for many years.
What are the risk factors for aortic valve stenosis?
Risk factors of aortic valve stenosis include: Older age. Certain heart conditions present at birth (congenital heart disease) such as a bicuspid aortic valve. History of infections that can affect the heart. Having cardiovascular risk factors, such as diabetes, high cholesterol and high blood pressure.
What are the four valves that keep blood flowing in the correct direction?
Your heart has four valves that keep blood flowing in the correct direction. These valves include the mitral valve, tricuspid valve, pulmonary valve and aortic valve. Each valve has flaps (cusps or leaflets) that open and close once during each heartbeat. Sometimes, the valves don't open or close properly. If a valve doesn't fully open or close, blood flow is reduced or blocked.
How many cusps does the aortic valve have?
However, some people are born with an aortic valve that has two cusps (bicuspid aortic valve). Your heart has four valves that keep blood flowing in the correct direction.
What is the name of the condition where the aortic valve is narrowed?
Aortic valve stenosis. In aortic valve stenosis, the aortic valve opening is narrowed (top row). The narrowing requires increased pressure within the heart to pump blood across a smaller opening. Eventually this reduces the heart's ability to pump blood to the body.
Can calcium buildup cause aortic valve stenosis?
The calcium deposits may never cause any problems. Aortic valve stenosis that's related to increasing age and calcium deposit buildup usually doesn' t cause symptoms until ages 70 or 80. However, in some people — particularly those with a congenital aortic valve defect — calcium deposits result in stiffening of the valve cusps at a younger age.
Can a bicuspid aortic valve be repaired?
The valve defect may not cause any problems until adulthood. If the valve begins to narrow or leak, it may need to be repaired or replaced. Calcium buildup on the valve.
Why do you need to perform AVR immediately after aortic valve replacement?
15 – 17 Because of the risk of sudden death, AVR should be performed promptly after the onset of symptoms.
What is the surgical option for AVR?
Surgical options for AS include AVR with a mechanical or bioprosthetic (heterograft) valve, AVR with an allograft (homograft) valve, pulmonic valve autotransplantation (Ross operation), aortic valve repair, and left ventricle–to–des cending aorta shunt ( Figure 2 ). Mechanical AVR designs include ball-and-cage valves, single tilting-disc prostheses, and bileaflet prostheses. 21 Bioprosthetic AVR can be stented or stentless and are reasonable in patients who want to avoid the risks and inconvenience of anticoagulation. Bioprosthetic valve durability is improving but may not be as good as a mechanical valve. Prosthetic valve complications include structural deterioration, symptomatic valve prosthesis–patient mismatch, thrombosis, embolism, bleeding complications from anticoagulation, endocarditis, tissue ingrowth, and hemolysis from periprosthetic aortic regurgitation.
Why are patients refused for AVR?
Patients may be refused for AVR because of high surgical risk (ST S score >10% or logistic EuroSCORE >20%) or coexisting noncardiac conditions that predict poor survival potential. Transcatheter valve implantation is intended for symptomatic patients with severe calcific AS requiring AVR who are at high risk for open heart surgery because of comorbid conditions and for patients who are inoperable. The Edwards SAPIEN valve system (Edwards Lifesciences Inc, Irvine, CA) is a trileaflet bovine pericardial valve mounted on a balloon-expandable stainless steel stent ( Figure 3 A). The second generation Edwards Sapien XT valve is mounted on a cobalt chromium stent frame. The CoreValve system (Medtronic, Minneapolis, MN) is a trileaflet porcine pericardial valve mounted in a self-expanding nitinol stent ( Figure 3 B). The devices are usually implanted by a transfemoral retrograde approach; the alternative is a transapical approach for the SAPIEN valve and a subclavian approach for the CoreValve. The devices are not approved for use in the United States but have been commercially available in Europe since 2007.
What are the future developments in the radial artery?
Future technical developments will include reduced device profile; better ways of measuring anatomic valve, aortic root, and peripheral artery dimensions; completely repositionable and retrievable devices; better percutaneous closure systems; and improved device durability. Cerebral protection devices delivered through the radial artery are in development. 25 More observational studies will be needed to improve patient selection and assess safety and durability. The potential of percutaneous valve-in-valve replacement may expand the use of bioprosthetic valves in younger patients. 26
Is endocarditis prophylaxis a statin?
Routine endocarditis antibiotic prophylaxis is no longer recommended. Although the active valvular disease process is characterized by lipid accumulation, inflammation, and calcification, statin therapy does not reduce disease progression in patients with severe AS. 9.
Is balloon aortic valvuloplasty a success?
Balloon aortic valvuloplasty was performed successfully, renal function normalized, and the patient subsequently became euvolemic with further therapy. After a short stay in a rehabilitation facility, she was discharged home and returned 1 month later to the cardiac surgery clinic for evaluation.
/slide016.jpg)
Diagnosis
Treatment
Clinical Trials
Lifestyle and Home Remedies

Specialist to consult
Preparing For Your Appointment