What are the best hypertension medications for African Americans?
· Thiazide diuretics may be particularly effective for African Americans as a dual therapy with one of the other commonly used medication classes. 11 The JNC 7 summary reads, “…African Americans…demonstrate somewhat reduced BP responses to monotherapy with BBs, ACEIs, or ARBs compared with diuretics or CCBs.
How do African Americans treat hypertension?
· Among African Americans with hypertension, the DASH diet was even more beneficial, reducing their systolic and diastolic blood pressure by 13.2 mm Hg and 6.1 mm Hg respectively. Another RCT studied the effect of different levels of dietary sodium in conjunction with the DASH diet.
Why is hypertension more common in African Americans?
The primary means of prevention and early treatment of hypertension in African Americans will be the appropriate use of lifestyle modification. The International Society of Hypertension in Blacks guidelines realize that most patients will require combination therapy, many of them first-line, to reach appropriate BP goals.
What are the 4 worst blood pressure drugs?
· What are the hypertension treatment options for African Americans? Experts recommend Black adults start with either a thiazide diuretic — such as chlorthalidone or hydrochlorothiazide — or a calcium channel blocker like amlodipine (Norvasc). If blood pressure readings are still too high after taking one of these medications for a while, providers will likely …

Which anti hypertensive medication is more effective in African Americans?
In the text of the guideline, mentions that diuretics should be the agent of first choice for blacks with hypertension because of their proven effectiveness in clinical trials. For whites, beta-blockers are also an option for first line therapy. Mono-therapy with beta-blockers or ACE-Is is less effective in blacks.
What is the first line antihypertensive for African American?
First-line pharmacologic treatment of hypertension for black patients includes thiazide diuretics or calcium channel blockers.
Why are ACE inhibitors not recommended for African black population?
Angiotensin converting enzyme (ACE) inhibitors have been avoided as an initial therapeutic option in the treatment of hypertension in African-Americans. A major reason for this has been the widespread perception of clinicians that these agents have poor blood pressure (BP) lowering efficacy in this population.
Is lisinopril a good blood pressure medicine for African Americans?
However, lisinopril was associated with an increased risk for heart failure (relative risk [RR] for African Americans=1.32; 95% CI, 1.11–1.58) and stroke (RR for African Americans=1.4; 95% CI, 1.17–1.68), and amlodipine was associated with a higher risk of heart failure (RR in African Americans=1.47; 95% CI, 1.24–1.74) ...
Is losartan good for African American?
Conclusions: The results of this study suggest that in African American patients, losartan monotherapy was significantly more effective than placebo in lowering SiSBP and SiDBP.
Is metoprolol good for African American?
Our study showed that metoprolol increased SUA and risk of GRM use in African American adults. This is consistent with other clinical studies involving beta blockers.
Why are calcium channel blockers preferred in African American?
The high efficacy of calcium blockers in patients of African ancestry points to enhanced vascular smooth muscle contractility in this group [11,12,36,37,39,72].
Are beta blockers good for African Americans?
It has been reported that beta blockers are not effective antihypertensives in black populations. A review of the literature revealed that, for the most part, studies drawing this conclusion were of small sample size, lacked controls, and did not represent the demographics of the US black population.
Do ACE inhibitors work on African Americans?
ACE inhibitor use in black patients had a statistically significant rate of poor cardiovascular outcomes (8.7% vs 7.7%), but this did not occur in white patients (6.4% vs 6.7%). Black patients who received ACE inhibitor treatment were no more likely to develop adverse effects than white patients.
Why are beta blockers less effective in African Americans?
Beta-blockers are generally less effective in Black hypertensives26 as a result of the tendency towards a low-renin state and a lower cardiac output, with increased peripheral resistance.
Abstract
Three large cohort studies determined that African Americans have a higher prevalence of hypertension and worse cardiovascular and renal outcomes when compared with white Americans.
Fingerprint
Dive into the research topics of 'What is the best treatment for hypertension in African Americans?'. Together they form a unique fingerprint.
Is there a clinical trial for BP?
There are no clinical trial data at present to suggest that lower-than-usual BP targets should be set for high-risk demographic groups such as African Americans. The primary means of prevention and early treatment of hypertension in African Americans will be the appropriate use of lifestyle modification.
Do black people have hypertension?
The prevalence of hypertension in blacks in the United States is among the highest in the world. Compared with whites, blacks develop hypertension at an earlier age, their average blood pressures are much higher and they experience worse disease severity.
Why are black people more likely to have hypertension?
There are multiple environmental factors that may contribute to higher rates of hypertension in Black adults in the U.S. For instance, Black adults and children are more likely than others to live in communities with less access to healthy foods and good healthcare. These communities are also less likely to have proper funding for physical education programs in schools and less likely to have spaces where people can exercise, such as playgrounds and public parks.
What is the best medication for high blood pressure?
In general, there are a few types of medications that are considered first choices for treating high blood pressure. These include thiazide diuretics (a type of “water pill”), angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), and calcium channel blockers (CCBs) .
How to keep blood pressure in check?
A healthy lifestyle can help keep hypertension in check. In fact, it’s almost always recommended you make diet and exercise changes — called lifestyle modifications — first to try to lower your blood pressure before taking medications. Some examples of these changes include:
What is high blood pressure?
High blood pressure — also known as hypertension — is when the force of blood pushing against the walls of your vessels (arteries) is consistently higher than what is considered safe. If your blood pressure is regularly 130/80 mm Hg or higher, you may have hypertension and should speak with your provider about ways to manage this, including lifestyle changes and medications.
How to lower blood pressure in adults?
Lifestyle changes like a healthy diet and regular exercise are effective and important techniques for lowering high blood pressure in all adults.
Why is blood pressure so high in black people?
We do not have a definite answer for why high blood pressure is more common in Black adults, but possible causes include genetic and environmental factors.
Do ACE inhibitors and ARBs work?
ACE inhibitors and ARBs both work by stopping the renin domino rally in the middle. While these medications don’t directly affect renin, they only work if higher levels of this hormone cause your hypertension. Because Black adults are more likely to have lower levels of renin, these two medication classes may be less effective at lowering blood pressure.
Do ACEIs help with congestive heart failure?
ACEIs have particular value in therapy for African-American hypertensives with concomitant congestive heart failure and may protect against progression of diabetic nephropathy. Finally, all hypertensives, especially African-American hypertensives, should have access to treatment prior to the development of end organ damage.
Is hypertension a diagnostic challenge?
The evaluation and treatment of hypertension in the African-American patient with an elevated blood pressure presents a diagnostic challenge . We are less able to rely on young age and resistance to treatment as indications for more extensive evaluation of secondary causes of hypertension; thus, grea …
What is HTN in blacks?
Blacks are especially susceptible to hypertension(HTN) and its associated organ damage leading to adverse cardiovascular, cerebrovascular and renal outcomes. Accordingly, HTN is particularly significant in contributing to the black-white racial differences in health outcomes in the US. As such, in order to address these health disparities, practical clinical practice guidelines (CPGs) on how to treat HTN, specifically in blacks, are needed. This review article is a timely addition to the literature because the most recent U.S. CPG more explicitly emphasizes race into the algorithmic management of HTN. However, recent clinical research cautions that use of race as a proxy to determine therapeutic response to pharmaceutical agents may be erroneous. This review will address the implications of the use of race in the hypertension CPGs. We will review the rationale behind the introduction of race into the U.S. CPG and the level of evidence that was available to justify this introduction. Finally, we will conclude with practical considerations in the treatment of HTN in blacks.
What is the biological profile of HTN in blacks?
The most recognized biological profile associated with HTN in blacks is the low renin physiology18. This physiology is associated with a salt-sensitive phenotype with excess effective circulating volume being the mechanism of HTN. This finding has been used to lend credence to the current strategy of using specific anti-HTN classes in blacks that address volume issues [ie. dihydropyridine calcium channel blockers (DHP-CCB) and diuretics]. While it appears that blacks tend to have a higher prevalence of low renin physiology than other racial/ethnic groups, caution must be taken to avoid the presumption that the distribution of renin activity in blacks is limited to the lower activity levels18. Furthermore, it should be appreciated that the low renin physiology cited usually refers to systemic renin activity, which has been shown to be often discordant with tissue renin activity19, which is arguably more important in terms of organ damage (eg intra-renal renin activity). Therefore, even though BP lowering may not be as robust with the “anti-renin” drugs (ie ACEIs/ARBs/Beta-blockers), the tissue-protective benefits should certainly be considered in the treatment of blacks in an effort to not only improve BP control but to achieve the ultimate goal of reducing the risk of organ damage.
Why is there a disparity in mortality between whites and blacks?
The stark disparity in over-all mortality between whites and blacks is largely a result of the disparate burden of HTN in black communities. As much as 30% of all deaths in HTN black men and 20% of all deaths in hypertensive black women might be attributable to high blood pressure(BP)9. HTN- related disease is especially severe in blacks10, 11and while there are similar treatment rates amongst the different racial/ethnic groups, HTN control rates are worse in blacks3. Several factors may contribute to the difficulty in achieving control in blacks:
What is personalized management of HTN?
Personalized management of HTN has been an explicit goal dating back to Joint National Committee (JNC)I13. Personalized medicine strives for “treatments targeted to the needs of individual patients on the basis of genetic, biomarker, phenotypic, or psychosocial characteristics that distinguish a given patient from other patients with similar clinical presentations”14.
Do blacks get HTN?
Given that HTN disproportionately affects the black population in the US3, blacks have been relatively under-represented in US HTN trial s. Even though the earliest Veteran Administration Cooperative Studies4, 5enrolled a relatively high proportion of blacks (>40%), these were smaller scale trials that do not represent modern day HTN therapy. Since these earlier trials, the more contemporary HTN trials have enrolled lower proportions of blacks (< 20%)6–8. It was only with the enrollment of a substantial proportion of blacks (35%) in the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) that the HTN guideline committees had good quality data on blacks with HTN with which to make recommendations/statements.
Is diuretic a first line agent?
Diuretics are recommended as first line agents in all hypertensives. JNC 7 mentions that diuretics are more effective at BP lowering in blacks than beta-blockers, ACE-I or ARBs. However, blacks with diseases such as chronic kidney disease and myocardial infarction benefit from ACE-I and beta-blockers. Consider the use of combination drug therapy that includes a thiazide type diuretic
Is race based therapy a branch point?
Race-based therapy in medicine has been gaining prominence in the new century and remains controversial2, 17, 20. The Report From the Panel Members Appointed to the Eighth JNC (henceforth referred to as ‘JNC 8’) only recently introduced race as a branch-point in the actual treatment algorithm in 2013. Prior to JNC 8, even though race was discussed within the text of previous JNC iterations, race was not a branch-point in published algorithms (Table 1).
What is the best treatment for African Americans with hypertension?
In African Americans with hypertension, therapy is best initiated with the low-sodium Dietary Approaches to Stop Hypertension (DASH) diet and a thiazide-type diuretic (strength of recommendation [SOR]: A, based on randomized controlled trials).
What is the blood pressure of African Americans?
Three large cohort studies determined that African Americans have a higher prevalence of hypertension and worse cardiovascular and renal outcomes when compared with white Americans. For African American patients, the standard blood pressure goals apply: below 140/90 mm Hg with uncomplicated hypertension and below 130/80 with diabetes or renal disease. 1
What is the name of the trial that shows the benefits of antihypertensive drugs?
The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial 4 (ALLHAT) and African American Study of Kidney Disease and Hypertension 5 (AASK) have demonstrated the benefit of blood pressure reduction using specific classes of antihypertensive agents.
How does the Dash diet affect blood pressure?
An RCT compared the effects of consuming the DASH diet (consisting of 4–5 servings of fruit, 4–5 servings of vegetables, 2–3 servings of low-fat dairy per day, and <25% fat) with a typical high-fat control diet among 459 adults with normal or elevated blood pressure. 2 Among 133 patients with hypertension, the DASH diet reduced systolic and diastolic blood pressure by 11.4 mm Hg (97.5% confidence interval [CI], –15.9 to –6.9) and 5.5 mm Hg (97.5% CI, –8.2 to –2.7) respectively when compared with the control diet. Among African Americans with hypertension, the DASH diet was even more beneficial, reducing their systolic and diastolic blood pressure by 13.2 mm Hg and 6.1 mm Hg respectively. 1
Do African Americans have lower blood pressure?
African Americans have reduced blood pressure responses to monotherapy with beta-blocker, ACE inhibitor, or ARBs when compared to diuretics or calcium channel blockers (SOR: A, randomized controlled trials). However, cardiac and renal indications for prescribing these medications should be equally applied to African American patients (SOR: C, expert opinion).
When was the first document to focus primarily on HTN in blacks or in any black population?
Accordingly, in March of 2003, the ISHIB published a consensus statement on the “Management of High Blood Pressure in African American,” 1 the first such document to focus primarily on HTN in blacks or in any black population.
What is the appropriate blood pressure control in diabetes?
In the placebo-controlled Appropriate Blood Pressure Control in Diabetes normotensive study, 34 patients with type 2 diabetes mellitus and BP <140/90 mm Hg were randomized to moderate BP control (DBP : 80 to 89 mm Hg; placebo) or intensive BP control (DBP: 10 mm Hg lower than baseline; active drug therapy). Baseline BP averaged 137/84 and 136/84 mm Hg, respectively, in the 2 treatment groups. Over ≈5 years, there was less progression of retinopathy and proteinuria and fewer strokes in the intensive-control group (BP averaged 128/75 mm Hg) compared with the moderate-control group (BP averaged 137/81 mm Hg). 34 In the Appropriate Blood Pressure Control in Diabetes hypertensive study 33 in patients with type 2 diabetes mellitus and DBP ≥90 mm Hg who were randomized to either intensive BP control (DBP: <75 mm Hg) or moderate BP control (DBP: 80 to 89 mm Hg), fewer overall deaths (5.5% versus 10.7%; P =0.037) occurred in the intensive BP control group. In the Hypertension Optimal Treatment Study, 37 there were fewer CVD events and myocardial infarctions and lower CVD mortality in the diabetic subgroup randomized to the ≤80-mm Hg treatment arm compared with the ≤90-mm Hg treatment arm. Thus, the totality of evidence, including the absence of substantive harm from aggressive BP lowering, was persuasive enough to leave unchanged the goal BP (<130/80 mm Hg) for nephropathy-, retinopathy-, and stroke-prone blacks with diabetes mellitus and HTN.
What are some non-biomedical beliefs about HTN?
A study of 93 blacks with HTN subjected to open-ended interviews during routine ambulatory clinic visits found that 38% believed that HTN could be cured, 38% believed that taking antihypertensive medication lifelong was not necessary, and 23% thought that antihypertensive medications needed to be taken only when experiencing symptoms. 64 Clearly, these beliefs could negatively influence the likelihood that blacks with HTN will seek treatment and, once prescribed, adherence to treatment over the long term.
How does diet affect HTN?
Diet and lifestyle likely play important roles in the pathogenesis of HTN in blacks and in the excess of HTN relative to whites. Blacks, especially women, are less physically active, consume more calories, and, not surprisingly, are more obese beginning in the preadult years than whites. 69,70 Blacks overall consume similar amounts of sodium but less potassium than whites. 71 Black hypertensive patients of higher socioeconomic status excrete significantly more urinary sodium and have higher urinary Na:K ratios than those of lower socioeconomic status. 72 Also, blacks residing in urban areas in the South excrete less urinary potassium and have higher urinary Na:K ratios than blacks residing in the urban Midwest. 73
What is the DBP for mild hypertension?
The Treatment of Mild Hypertension Study showed that treatment (with 1 of 5 different antihypertensive drug regimens) plus multifactorial lifestyle modification compared with multifactorial lifestyle modification alone in men and women aged 45 to 69 years (20% black) with diastolic BP (DBP) <100 mm Hg (baseline BP: 140/91 mm Hg) reduced the risk of the aggregate end point of pressure-related complications when SBP was lowered to ≈126 mm Hg (lifestyle modification plus active drug) versus ≈132 mm Hg (lifestyle modification alone). 132 Clinical event rates were 16.2% (lifestyle modification only) versus 11.1% (active drug treatment) ( P =0.03), and quality of life was also improved more in the active drug treatment group. The Cardio-Sis study, another prospective, randomized trial, was conducted in 1111 European nondiabetic men and women with SBP ≥150 mm Hg plus 1 additional CVD risk factor at entry to determine whether a target SBP <130 mm Hg (tight control) was superior to SBP <140 mm Hg (usual control). 133 After a median 2-year follow-up, the rate of ECG-LVH (primary end point) was 37% lower ( P =0.013) in the tight-control group compared with the usual-control group; the secondary composite CVD end point was also lower (9.4% versus 4.8%; P =0.003) in the tight-control group. The attained BP level at the end of 2-year follow-up was 131.9/74.0 in the tight-control group versus 135.6/78.7 mm Hg in the usual-control group (72.2% versus 27.3% achieved BP <130/80 mm Hg). 133 Pharmacological treatment of prehypertensive middle-aged (48.5 years) individuals in the Trial of Preventing Hypertension reduced the incidence of frank HTN by 66.3% ( P <0.001) at 2 years and by 15.6% ( P <0.007) at 4 years compared with placebo. 134 Finally, in the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT), the best study outcomes overall were obtained with chlorthalidone, in which group BP averaged 134/76 mm Hg at 4.9-year follow-up. 135 Collectively, these studies suggest the likely benefits of pharmacological treatment of HTN in lower risk hypertensive patients to BP levels lower than those currently recommended by JNC 7 or other organizations. Thus, our new recommendation is to maintain BP persistently <135/85 mm Hg in patients who do not have evidence of target organ damage, preclinical CVD, or overt CVD. In such patients, if BP is <145/90 mm Hg in the absence of target-organ injury or other risk-enhancing comorbidities, ≤3 months of comprehensive lifestyle modification may be attempted without concurrent drug therapy (see Figure 1 ).
What is the emphasis of the ISHIB consensus statement?
The emphasis in this updated ISHIB consensus statement is on the interpretation of the BP response and clinical end point data and how these observations mesh with the totality of the evidence available for consideration. We strongly encourage practitioners to diagnose, stratify risk, and treat blacks on an individualized basis rather than to make blanket extrapolations regarding preferred antihypertensive drugs to all blacks.
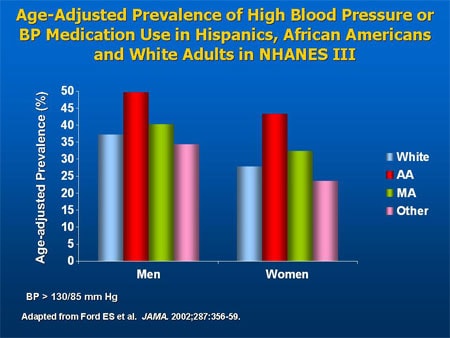
What was the prevalence of HTN in 2006?
The age-adjusted prevalence of HTN during 2006 among individuals aged ≥20 years in the total US population was 33.3% (73 600 000). 49 Non-Hispanic blacks had the highest age-adjusted prevalence (44.4% men and 43.9% women), non-Hispanic whites an intermediate prevalence (34.1% men and 30.3% women), and Mexican Americans the lowest prevalence (23.1% men and 30.4% women). In a different analysis among children aged 8 to 17 years in 1999–2000, systolic BP (SBP) levels were 2.9 and 1.6 mm Hg higher in non-Hispanic black boys and girls, respectively, than in age-matched non-Hispanic whites, a finding attributable in part to an increased prevalence of overweight in black children. 50
What is the best medicine for high blood pressure in African Americans?
Recommended Medications for High Blood Pressure in African-Americans. Calcium Channel Blockers (CCB’s) Calcium Channel Blockers (CCB’s) are recommended for first line use for African Americans by JNC 8. They should be used in combination with Thiazide Diuretics. Some are listed below by generic name: Nifedipine.
What is ACE inhibitor?
ACE Inhibitors are used with Calcium Channel Blockers and Thiazide Diuretics for chronic kidney disease and high blood pressure in African Americans.
Why are black people more likely to have PA?
Black people are also more likely to have PA as a result of bilateral adrenocortical hyperplasia with suppressed PRA levels and inappropriately elevated levels of plasma aldosterone in relation to renin. 10
What are the two streams of low renin hypertension?
There are 2 streams of low-renin hypertension: low renin/low aldosterone (Liddle phenotype) attributable to overactivity of the renal tubular ENaC and low renin/high aldosterone (primary aldosteronism/inappropriate aldosterone secretion [PA] phenotype), and there are variants of at least 6 genes that predispose to each of these 2 phenotypes. 7 Although true Liddle syndrome (resulting from variants of SCNN1B [ENaC]) is rare, the phenotype is common, as discussed below, because the other variants are common.
Why is the Jackson Heart Study important?
In conclusion, this report from the Jackson Heart Study is important because it links suppressed renin to the pathogenesis of hypertension in Black patients , with a higher prevalence of a Liddle phenotype than previously recognized.
Is amiloride good for PA?
The importance of distinguishing between these phenotypes is that amiloride, an ENaC inhibitor, is the preferred treatment for the Liddle phenotype, whereas aldosterone antagonists are best for the PA phenotype. In patients with uncontrolled hypertension, physiological individualized therapy in Black patients in Africa has been shown to substantially improve BP control. 11 In a study of physiological individualized therapy versus usual care in patients in Africa with uncontrolled hypertension, physiological individualized therapy markedly improved BP control. At the Nigerian site, where patients were randomized and had access to amiloride and clinic visits, systolic control was obtained in 15% of those receiving usual care versus 85% of those receiving physiological individualized therapy ( P =0.0001), diastolic control was obtained in 45% versus 75% ( P =0.11), and control of both systolic and diastolic BPs and was obtained in 15% versus 75% ( P <0.0001), although renal function was worse at that site.
Does aldosterone affect BP?
However, the relationship between aldosterone and BP was not particularly strong. A higher log-aldosterone was associated only with higher clinic, awake, and asleep diastolic BP (all P <0.05). There was no relationship with systolic BP. However, given the bimodal relationship of aldosterone with low-renin hypertension, this finding is not unexpected. In the total cohort, there were 646 subjects with PRA results; of these, 103 (15.9%) subjects had the typical Liddle phenotype defined by PRA <0.5 ng·mL −1 ·h −1 and aldosterone in the lowest quartile (1.9–2.7 ng/dL), and 60 (9.3%) had the typical PA phenotype defined by low renin with aldosterone in the highest quartile (7.6–61.1 ng/dL). Perhaps it would have been more informative to report BP and ABP in relation to these 2 phenotypes.
