Treatment
- In situ fixation. Classical treatment of SCFE consists in percutaneous fixation of the epiphysis. ...
- Prophylactic pinning. Bilateral involvement in SCFE ranges from 14% to 63%, depending on the studies considered. ...
- Compensatory osteotomies. ...
- Surgical hip dislocation (SHD) An important role is played by SHD, also called the modified Dunn procedure. ...
What is SCFE (SCFE)?
SCFE is the most common hip disorder in adolescents. In SCFE, the epiphysis, or head of the femur (thighbone), slips down and backwards off the neck of the bone at the growth plate, the weaker area of bone that has not yet developed.
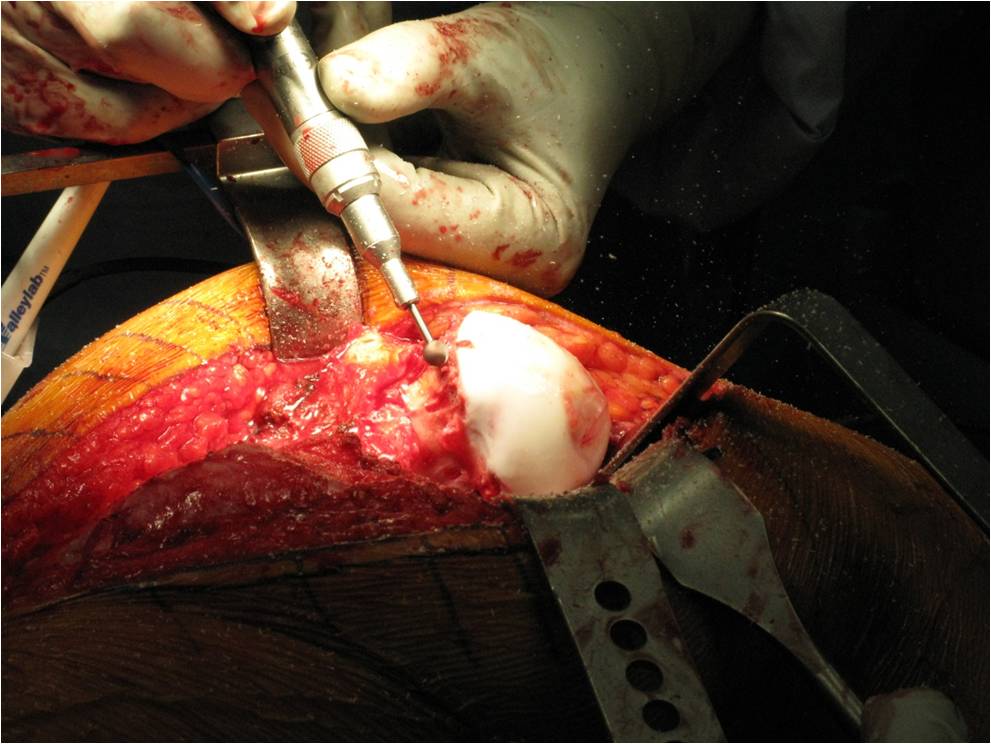
What is in situ fixation for SCFE?
In situ fixation. This is the procedure used most often for patients with stable or mild SCFE. The doctor makes a small incision near the hip, then inserts a metal screw across the growth plate to maintain the position of the femoral head and prevent any further slippage. Over time, the growth plate will close, or fuse.
Why is it important to be diagnosed of SCFE early?
To achieve the best outcome, it is important to be diagnosed as quickly as possible. Without early detection and proper treatment, SCFE can lead to potentially serious complications, including painful arthritis in the hip joint. Anatomy The hip is a ball-and-socket joint.
What are the different types of SCFE?
Types of SCFE include: 1 Stable SCFE. In stable SCFE, the patient is able to walk or bear weight on the affected hip, either with or without... 2 Unstable SCFE. This is a more severe slip. The patient cannot walk or bear weight, even with crutches. Unstable SCFE... More ...

Can SCFE be cured?
In all cases, children with a SUFE need surgery. It is very important that your child avoids standing up and placing weight on their leg until the SUFE is corrected surgically, so until then they will need to use a wheelchair or have bed rest.
What is SCFE caused by?
The exact cause of SCFE is not known. There are, however, many factors that are associated with this condition. These factors lead to weakening of the growth plate (also called the “physis”) which then causes the femoral head (ball of the femur) to slip off the neck of the femur. Obesity is a major risk factor.
How long does it take to recover from SCFE surgery?
Activity. After the surgery, your child will need crutches or a walker for about 4 to 6 weeks. The type of SCFE and the surgical procedure done will determine your child's weight-bearing status on the operated leg. A physical therapist will teach your child how to use crutches before he goes home.
What happens if SCFE is not treated?
Untreated SCFE may result in progressive deformity and pain, destabilization of the femoral epiphysis, and decreased range of motion of the hip joint.
What are the symptoms of SCFE?
Symptoms of SCFE typically include complaints of pain in the groin or hip that is aggravated by activity. Sometimes the child will also experience pain in the thigh or knee area. In acute or unstable slips, the child will complain of immediate pain, limp, or feel like the leg is "giving way."
Is SCFE an emergency?
SCFE is usually an emergency and must be diagnosed and treated early. In 20 to 40 percent of affected children, SCFE will be present in both hips at the time the child is diagnosed. If only one hip is affected, the other hip will eventually slip 30 to 60 percent of the time. Treatment is surgical.
Is SCFE surgery painful?
The pain is similar to what might be felt with a broken bone. The child probably won't be able to move the injured leg. If you think your child has unstable SCFE, don't force the leg to move. That could make the thigh bone slip even more.
How painful is SCFE?
A stable SCFE causes some stiffness or pain in the knee or groin area, and possibly a limp that causes a child to walk with a foot outward. The pain and the limp may come and go, and may get worse with activity and better with rest. With a stable SCFE, a child still can walk, even if they need to use crutches.
Is SCFE a disability?
SCFE occurs through the unfused growth plate of the proximal femur where the femoral head slips posteriorly on the femoral neck. Serious consequences of the problem, such as gait disturbance, post-traumatic arthritis, chondrolysis and osteonecrosis of the femoral head can occur, leading to lifelong disability.
How is SCFE diagnosed?
Patients with SCFE usually present with limping and poorly localized pain in the hip, groin, thigh, or knee. Diagnosis is confirmed by bilateral hip radiography, which should include anteroposterior and frog-leg views in patients with stable SCFE, and anteroposterior and cross-table lateral views in unstable SCFE.
What is the most common age range for slipped capital femoral epiphysis?
SCFE usually occurs in those eight to 15 years of age and is one of the most commonly missed diagnoses in children. SCFE is classified as stable or unstable based on the stability of the physis.
What is a scfe?
Slipped Capital Femoral Epiphysis (SCFE) Slipped capital femoral epiphysis (SCFE) is a hip disorder. The head of the femur slips off the neck of the bone at the growth plate. Typically, SCFE occurs in overweight children between 11 and 16 years old.
How to diagnose SCFE?
SCFE is diagnosed through physical exam including rotation of the affected leg, observation while walking and X-rays. A MRI may be ordered if the diagnosis is not able to be made with X-rays and your healthcare provider still suspects your child has SCFE. Your provider may also order blood work to check for other medical conditions.
How long does it take for a child to recover from a scfe?
Your healthcare provider will discuss your child’s expected time to full recovery. It’s unique to each child and depends on many factors including severity of SCFE and type of surgical procedure done. In general, expect that your child will need crutches or a walker for up to about four weeks after surgery for stable SCFE and for at least six to eight weeks for unstable SCFE. Your child will work with a physical therapist to help strengthen leg and hip muscles and improve range of motion. Talk with your provider about when your child can return to normal activities including sports.
How to tell if a teen has slipped capital femoral epiphysis?
Symptoms of slipped capital femoral epiphysis include: Pain in your teen’s groin, knee or hip. Stiffness in your teen’s hip. Foot/leg that is turned outward. Walking with a limp. Can’t put weight on the leg (usually in more severe cases and with extreme pain). One leg may look shorter than the other.
How long after scfe surgery do you need crutches?
In general, expect that your child will need crutches or a walker for up to about four weeks after surgery for stable SCFE and for at least six to eight weeks for unstable SCFE. Your child will work with a physical therapist to help strengthen leg and hip muscles and improve range of motion.
Where is the SCFE bone located?
The growth plate is where new bone forms. It’s located in the ‘neck’ area of the femur between the “ball” section and the long shaft section of the femur.
What is unstable SCFE?
Unstable SCFE: This type is more severe. Your child will not be able to put weight on the affected leg . This type tends to happen suddenly and is more painful. It can also lead to more serious complications.
What is the result of SCFE?
The first is “ osteonecrosis .” “Osteo” means bone and “necrosis” means death. In osteonecrosis, the blood supply to the femoral head is damaged and the bone dies.
What are the complications of SCFE?
The first is “ osteonecrosis .” “Osteo” means bone and “necrosis” means death . In osteonecrosis , the blood supply to the femoral head is damaged and the bone dies. This can lead to degenerative joint disease ( osteoarthritis ). The other complication is called “chondrolysis”. “Chondro” means cartilage and “lysis” means cutting apart. In this complication, the joint cartilage is damaged and leads to a painful and stiff joint.
What is a slipped capital femoral epiphysis?
Slipped capital femoral epiphysis (SCFE) a disorder of adolescents in which the growth plate is damaged and the femoral head moves (“slips”) with respect to the rest of the femur. The head of the femur stays in the cup of the hip joint while the rest of the femur is shifted.
What is the treatment for SCFE?
There are two methods for treating SCFE: In situ pinning – The aim of this surgery is to secure the hip in its current position and prevent further slipping.
What is FAI in scfe?
What is FAI and how does it relate to SCFE? FAI stands for femoroacetabular impingement and refers to a mismatch between a deformed femoral head from SCFE and the acetabulum. The slipped epiphysis leads to the ball not moving in a normal fashion and causing the femur to impinge on the acetabulum during normal motion.
How to secure epiphysis to femur?
One or two screws are placed through the skin through a small incision into the femoral head to secure the epiphysis to the femur. Open surgery – This surgical procedure is used for patients with unstable SCFE to align the epiphysis on the femur and attempt to prevent the loss of blood flow to the femoral head.
What is the expected short term outcome after SCFE surgery?
The expected short-term outcome after SCFE surgery is a return to full activity without pain. The amount of slipping of the epiphysis, or the degree of deformity to the femoral head, affects the amount of limitation in range of motion and activity.
How long do you have to be on crutches after SCFE?
Children are usually on crutches for six weeks after in situ pinning and 12 weeks after open surgery. The expected short-term outcome after SCFE surgery is ...
Can you get SCFE in the other hip?
Yes, it is possible for SCFE to happen to the other hip. The risk for it occurring depends on many variables, but it is important that if pain begins to happen in the other hip that the patient seeks immediate medical attention.
What is the procedure for SCFE?
Testing and diagnosis. In addition to a complete medical history and physical examination, diagnostic procedures for SCFE almost always include X-rays, which use invisible electromagnetic energy beams to produce images of the bone onto film.
Who determines the treatment for SCFE?
Specific treatment for SCFE will be determined by your child's doctor based on:
How to tell if a child has SCFE?
Signs and symptoms. Symptoms of SCFE typically include complaints of pain in the groin or hip that is aggravated by activity. Sometimes the child will also experience pain in the thigh or knee area. In acute or unstable slips, the child will complain of immediate pain, limp, or feel like the leg is "giving way.".
What is a slipped capital femoral epiphysis?
What is slipped capital femoral epiphysis? Slipped capital femoral epiphysis (SCFE) is a condition of the hip joint that affects adolescents. In SCFE, the head, or "ball," of the thigh bone (referred to as the femoral head) slips off the neck of the thigh bone. An analogy commonly used to describe this condition is that it can be like a scoop ...
What is the pain of SCFE?
Unstable: In this type of SCFE, the pain occurs suddenly, almost like a break. Pain is usually severe and patients can’t walk, not even with crutches. Because this type of SCFE occurs suddenly, the blood flow can be affected 20 to 50 percent of the time which can result in the bone dying ( avascular necrosis ).
When does a scfe start?
SCFE develops most often during short periods of accelerated growth following the onset of puberty. SCFEs can be divided into two major types:
What are the risk factors for SCFE?
Risk factors that increase the likelihood of SCFE include the following: Risk factors may include: Obesity. Medications (such as steroids) Thyroid problems. Radiation treatment. Bone problems related to kidney disease.
How long does AVN last after SCFE?
AVN is more likely to occur in patients with unstable SCFE. Because evidence of AVN may not be seen on x-ray for up to 12 months following surgery, the patient will be monitored with x-rays during this period of time. Chondrolysis. Chondrolysis is a rare but serious complication of SCFE.
How to treat displaced femoral head?
The goal of treatment is to prevent the displaced femoral head from slipping any further. This is accomplished by surgical stabilisation of the hip. Early diagnosis gives the best chance of stabilizing the hip and avoiding complications. When treated early and appropriately, long-term hip function can be expected to be very good. Once SCFE is confirmed, your child will not be allowed to bear weight on his or her hip and will be admitted to the hospital for surgery.
Does SCFE help with complications?
Although early detection and proper treatment of SCFE will help decrease the chance of complications, some patients will still experience problems.
What is a SCFE?
Description: Traditionally slipped capital femoral epiphysis (SCFE) has been described as posterior and medial slippage of the capital femoral epiphysis with respect to the metaphysis. However, the epiphysis is held in the acetabulum by the ligamentum teres; thus, the metaphysis actually moves laterally and anteriorly in relation to the epiphysis.
What is SCFE in a femoral?
Typical SCFE involves posterior and medial slippage of the proximal femoral epiphysis relative to the metaphysis (anterior and lateral slippage of the metaphysis relative to the epiphysis).
How to calculate SCFE?
Calculated by measuring the abnormal side and subtracting the measurement on the unaffected side (or subtracting the average normal of 12 degrees in the case of bilateral SCFE) (Southwick 1967).
Is SCFE multifactorial?
The etiology of SCFE is thought to be multifactorial with a combination of both biochemical and biomechanical contributing forces. There is an increased risk of SCFE in patients with renal disease, endocrine abnormalities (hypothyroidism, hyperparathyroidism), radiation to the hip/pelvis, Down syndrome.
How long does SCFE last?
Chronic SCFE represents the major part of the disease (around 85%): symptoms are present for >3 weeks, with remission and relapse.
What causes a SCFE?
On the other hand, metabolic causes implicated in SCFE are obesity,10some endocrinological diseases, such as hypothyroidism and kidney failure, and treatment with growth hormone. 5As previously reported, the onset of SCFE usually occurs during the period of maximum growth, but the age of onset is continuously changing, as there has recently been a tendency for this period to occur earlier.11Most case series have reported bilateral involvement in as many as 63% of patients,2underlining the importance of metabolic factors. Kohno et al found that ~70% of contralateral hips in unilateral SCFE patients had a subclinical posterior inclination of the capital femoral epiphysis, indicating the possibility of bilateral involvement. The contralateral posterior sloping angle was a reliable predictor of a contralateral slip, and an angle of 19° was the cutoff value for developing SCFE.12
What is the AVN rate in SCFE?
Several studies have focused on this issue, reporting AVN rates of 6%–58% in treated unstable SCFE, while the rate has been reported to be close to zero in treated stable SCFE . Factors related to the development of AVN include unstable hips with separation of the epiphysis from the metaphysis, delay from presentation to surgery, severity of the slip, younger age, short duration of prodromal symptoms, increased intracapsular pressure, and choice of surgical technique. The etiology of AVN is well understood, multifactorial, and includes several causes for an interruption in blood supply to the femoral head. It goes from an increase in capsular pressure leading to reduced blood flow to the epiphysis to compression, overstretch, kinking, or tearing of posterior retinacular blood vessels at the time of injury or during reduction and fixation of the dislocated epiphysis.20
What are the antecedents of SCFE?
Antecedents include greater retroversion of the femoral neck or a coxa profunda5related to major weakness of the growth plate during the period of rapid growth.6 Gebhart et al examined the differences in two common anatomic measurements – pelvic incidence (PI) and acetabular retro-version – and their associations with post-SCFE deformity. They claimed that in a patient with a small PI, the pelvis will often tilt forward to maintain normal lumbar lordosis and balance sagittal alignment of the spine. Such anterior tilt would load the anterior aspect of the hip joint and deliver the stress across the physis of the proximal femur. This increased stress, along with other mechanical insults, such as obesity, physeal sloping angle, femoral retroversion, and size of the epiphyseal tubercle, could potentially result in the development of an SCFE. Their study demonstrated that specimens with SCFE deformity have a smaller PI than a large cohort of normal control specimens. On the contrary, they did not find significant differences between acetabular versions of specimens with and without SCFE deformity. The unaffected acetabulum of SCFE specimens was not more retroverted than the affected side.7
When is SCFE radiography needed?
Radiography is needed when patients 8–15 years of age complain of new-onset limping and lower-limb pain. When SCFE is suspected, radiography should include anteroposterior and frog-leg views of both hips. In unstable SCFE, such imaging should be compared to the unaffected side. Several radiographic signs are suggestive of SCFE, such as widening of the physis, relative decreased height of the epiphysis, loss of intersection of the epiphysis by a lateral cortical line along the femoral neck (Klein’s line) and double density detected at the metaphysis (Steel sign, which is caused by posterior slip of the epiphysis).15–17
What is unstable SCFE?
A patient with unstable SCFE, however, often has severe hip pain that does not allow gait. Medical history is often positive for hip, thigh, and knee pain and previous trauma (of a minor entity that does not justify the condition). The patient lying on the couch has an attitude in external rotation of the side affected and counteracts any passive movement of the hip. Obligatory external rotation of the hip is noted when it is passively flexed to 90°. Although it is complicated to assess the rate of unstable SCFE, it is estimated to be around 10%–35% of patients presenting with such a condition.
What is a slipped capital femoral epiphysis?
Slipped capital femoral epiphysis (SCFE) is a common hip disorder in children and adolescents, and it consists in posteroinferior migration of the epiphysis in metaphysis through the physis in proximal femur. The current incidence of SCFE ranges from 0.33 in 100,000 to 24.58 in 100,000 children 8–15 years of age, depending upon sex and ethnicity.