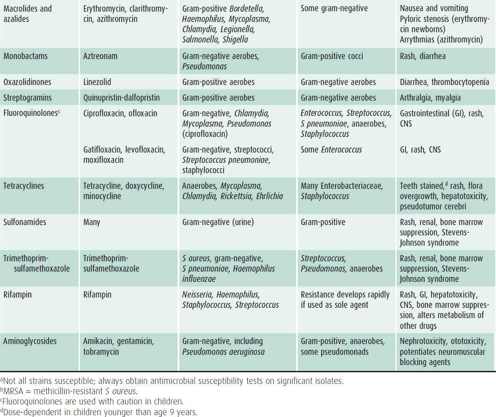
Common antimicrobials
| Antibiotic | Stability at 25 °C | Diluent | Existing data in elastomeric pumps |
| cefepime | 24 hours | normal saline | Yes |
| ceftazidime | 48 hours | normal saline | Yes |
| clindamycin | 16 days | dextrose 5% | No |
| flucloxacillin | 24 hours | normal saline | Yes |
What prevents the intravenous to oral antibiotic switch?
Results
- Consumerism and ‘complaints culture’. Participants described the significant role of patients in influencing their choice of iv versus oral antibiotics.
- Priorities, team dynamics and the medical hierarchy. ...
- Mythical properties of intravenous antibiotics: ‘iv anything is better than oral …’. ...
- Supplementary data. ...
What are the different types of intravenous antibiotics?
Top 10 List of Brand Name Antibiotics
- Augmentin
- Flagyl, Flagyl ER
- Amoxil
- Cipro
- Keflex
- Bactrim, Bactrim DS
- Levaquin
- Zithromax
- Avelox
- Cleocin
Is penicillin a good antibiotic?
Prescription antibiotics, such as penicillin, have helped people to recover from otherwise fatal diseases and conditions since the 1940s. However, people are also turning to natural antibiotics for treatment. According to the NHS, 1 in 10 people experiences side effects that harm the digestive system after taking antibiotics.
How do antibiotics such as penicillin stop bacterial growth?
What are 4 possible side effects of using antibiotics?
- vomiting.
- nausea (feeling like you may vomit)
- diarrhoea.
- bloating and indigestion.
- abdominal pain.
- loss of appetite.

What's the difference between oral and IV antibiotics?
Intravenous (IV) antibiotics are used for: Severe life-threatening infections, such as sepsis. Deep seated infections in parts of the body where oral antibiotics are less effective, such as in the spinal fluid and bone. Infections resistant to oral antibiotics.
What is IV antibiotic therapy?
Antibiotic Infusion Therapy allows patients to avoid hospitalization for severe infections by receiving intravenous (IV) antimicrobial therapies in a clinic or at home. IV antibiotics are antibiotics that are administered directly into a vein to enter the bloodstream immediately and bypass the absorption in the gut.
How are IV antibiotics given?
When long courses of IV antibiotics are given outside the hospital, they are administered through a small tube called a catheter placed in a large vein, usually on the inside of the upper arm. A sterile protective dressing is placed over the catheter insertion site.
What conditions require IV antibiotics?
Infections that may be suitable for a short course of intravenous antibiotic include pneumonia, complicated urinary tract infections, certain intra-abdominal infections, Gram-negative bacteraemia, acute exacerbations of chronic lung disease, and skin and soft tissue infections.
What is the strongest antibiotic through IV?
Vancomycin is used to treat serious bacterial infections. It is an antibiotic that works by stopping the growth of bacteria. This medication is usually given by injection into a vein.
How long are you in the hospital for IV antibiotics?
The optimal duration of intravenous antibiotic therapy is not clearly defined. Individuals usually receive intravenous antibiotics for 14 days, but treatment may range from 10 to 21 days. A shorter duration of antibiotic treatment risks inadequate clearance of infection which could lead to further lung damage.
Do you have to stay in the hospital for IV antibiotics?
IV antibiotics may also be administered in infusion centers, which serve patients who prefer to receive their IV antibiotics in a clinical setting without being hospitalized. Patients who require a higher level of care may complete their therapy in a skilled nursing facility (SNF).
What are the side effects of IV antibiotics?
The most common side effects associated with using IV antibiotics include rash, itch, diarrhea....Call your doctor, nurse, or healthcare professional if you have these signs of infection:Redness, swelling or bruising at the site where the needle enters the vein.Pain.Bleeding.Fever over 100.5 °F (38.0 °C)
How long IV antibiotics take to work?
Antibiotics begin to work right after you start taking them. However, you might not feel better for 2 to 3 days. How quickly you get better after antibiotic treatment varies. It also depends on the type of infection you're treating.
What is the strongest antibiotic a doctor can prescribe?
Prescriptions of the extremely powerful antibiotic vancomycin—one of the only drugs effective against the scary skin infection, methicillin-resistant Staphylococcus aureus (MRSA)—increased by 27 percent.
Are intravenous antibiotics stronger?
Among physicians and patients alike, it is generally accepted that IV antibiotics are better than oral. They are stronger. They will work faster. They will save the day when oral antibiotics have failed.
What is OPAT?
OPAT is the administration of intravenous (IV) antibiotics outside of an acute care hospital, such as in a skilled nursing facility, outpatient infusion center, or in the home.
Johns Hopkins Bayview Medical Center OPAT Clinic
The Infectious Disease Division has an integrated OPAT management program for patients discharged from Johns Hopkins Bayview Medical Center. This means patients will be managed by a team of specialists from both Johns Hopkins Bayiew Medical Center and Johns Hopkins Hospital depending on which antibiotics patients need.
Johns Hopkins Bayview Medical Center
William F Wright, DO, MPH leads the Johns Hopkins Bayview OPAT clinic. Other physicians with a special clinical interest in OPAT include Mamuka Machaidze, MD; and Sara Karaba, MD, PhD. The Johns Hopkins Bayview Medical Center OPAT clinic is located at:
Rockland Physician Practice at Greenspring Station
Sara Keller, MD, MPH, MSPH leads the Greenspring OPAT clinic. Other physicians with a special clinical interest in OPAT include Christopher Lippincott, MD, MPH ; Maryana Shenderov, MD; and Mamuka Machaidze, MD and William Wright, DO, MPH . The Johns Hopkins Rockland Physician Practice at Greenspring is located at:
John G. Bartlett Specialty Practice
Sara Keller, MD, MPH, MSPH leads the Bartlett OPAT clinic. Other physicians with a special clinical interest in OPAT include Christopher Lippincott, MD, MPH; Maryana Shenderov, MD; Karen Coffey, MD, MPH; Juhi Moon, MD; Mamuka Machaidze, MD; and William Wright, DO, MPH. The John G. Bartlett Specialty Practice is located at:
Clinical Excellence Award
In response to post-discharge safety issues, Johns Hopkins Bayview formed a multidisciplinary team to improve tracking and care coordination for patients on IV antibiotics.
What is the best parenteral regimen for community use?
The preferred parenteral regimens for community and first-level facility use are a combination of procaine penicillin G and gentamicin, or ceftriaxone given alone, which are safe and retain efficacy when dosed at extended intervals (≥24 hours) by intramuscular administration.
What is the best antibiotic for neonatal sepsis?
Ampicillin has been widely used in neonatal medicine as empiric therapy for early-onset neonatal sepsis and meningitis, in combination with gentamicin for synergistic activity against Group B Streptococcus (GBS), enterococci, Listeria monocytogenes, and some Enterobacteriaceae (eg, Enterobacter spp., Proteus spp., Escherichia coli ). 2 Ampicillin and gentamicin (see later in the text) continue to be the first-line, standard-of-care antibiotics for treatment of neonatal sepsis in developing as well as developed countries. 2–4 Although ampicillin remains the first-line antibiotic of choice for use in health-facilities, use in community -based settings is not feasible because of the need to administer doses more frequently than once daily. Furthermore, increasing ampicillin resistance among Gram-negative rods has developed worldwide. 2,5,6 Klebsiella spp. are intrinsically resistant to ampicillin , and most strains of Staphylococcus aureus are now also resistant. 7
What is the best antibiotic for a staphylococcal infection?
The combination of parenteral oxacillin (or nafcillin) and gentamicin is widely recommended for empirical treatment of suspected serious staphylococcal infections, for example when umbilical or skin infection, or a consolidated pneumonia suspicious for S. aureus, is identified as the potential source for invasive disease, in addition to some late-onset neonatal infections. 2 These antimicrobials can also be used to treat infections caused by streptococci, including Group B streptococcal and pneumococcal infections; however, the natural penicillins are preferred. 10 The antistaphylococcal penicillin alone, however, lack activity against enterococci or Gram-negative bacilli. Nafcillin is preferred for central nervous system (CNS) infections. Antistaphylococcal penicillins are safe and well tolerated in neonates, although occasional cases of nephrotoxicity (due to large doses of methicillin) and hepatotoxicity (due to oxacillin) have been described. 2 Moreover, repeated IM dosing of these agents may result in muscle damage. Half-life is prolonged in neonates <7 days old and dosing intervals of 12 hours are adequate. 18 Oral cloxacillin is commonly used for the treatment of superficial skin and umbilical cord infections in developing countries; however, there is no experience with using oral cloxacillin in the treatment of invasive neonatal infections. Frequent dosing, lack of CSF penetration, and narrow spectrum of activity (eg, not active against enterococci or Gram-negative bacilli) are limitations for home-based therapy. Methicillin resistant S. aureus is reported as a significant pathogen in hospital-based studies in India and elsewhere in low resource settings 6,19,20; however, it is unclear if methicillin resistant S. aureus is a problem in the community, although limited data suggest this may be so (Darmstadt GL, unpublished data).
Is chloramphenicol safe for neonates?
2 Today, because of safer alternatives, use of chloramphenicol is largely restricted to developing countries where third generation cephalosporins are used infrequently because of their expense. Chloramphenicol is cheap, has broad-spectrum activity, and excellent CNS penetration. 2 It is bactericidal against H. influenzae and S. pneumoniae, but bacteriostatic against GBS and most Gram-negative enteric rods. 2 Large variability in serum concentrations and half-lives after both oral and IV administration has been reported by many investigators. 21–29 Therefore, monitoring of serum levels to guide dosage is necessary to avoid subtherapeutic or potentially toxic levels. 2,30,31 Concentrations in CSF are 35% to 90% of those in the serum, regardless of meningeal inflammation. 29,32 Oral administration of chloramphenicol in neonates results in much lower serum concentrations than those observed after IV or IM administration, and wide fluctuations in levels have been observed in neonates given the same dosage, perhaps because of immaturity of the neonatal gastrointestinal tract and resultant erratic absorption. 21,25,26
Is procaine penicillin good for syphilis?
There is substantial experience in using longer-acting procaine penicillin G administered intramuscularly (IM) to ne onates with sepsis and congenital syphilis. 2,11,12 Procaine penicillin provides excellent coverage against GBS, Group A streptococci, meningococci, Treponema pallidum, L. monocytogenes, and most strains of Steptococcus pneumoniae. Procaine penicillin combined with an aminoglycoside, administered IM, is used as empiric first-line treatment of neonatal sepsis in some developing countries, especially in areas where difficulty in establishing venous access precludes use of intravenous (IV) ampicillin. This regimen is also used in neonatal IMCI protocols in some countries. The penicillin agents exhibit synergy with aminoglycosides against GBS as well as S. aureus, enterococci, and Listeria. However, ampicillin is preferred over penicillin when venous access and multiple daily dosing are not problematic because of its wider spectrum of activity with an equivalent safety profile and better CSF penetration.
Is cephalosporin safe for neonates?
For community -based management of neonatal infections, particularly attractive properties include efficacy and safety of extended-interval, intramuscular dosing regimens. The penicillins and cephalosporins have relatively favorable effica cy and safety profiles. Although the aminoglycosides have narrow therapeut ic indices, when used appropriately, they are safe and effective. Although inexpensive and effective, the potential for significant life-threatening toxicity among neonates associated with chloramphenicol makes it the least preferred of the parenteral agents for empiric therapy.
Does gentamicin work against GBS?
Aminoglycosides, including gentamicin, have been widely used as first-line therapy for neonatal infections, primarily because of their excellent spectrum of activity against Gram-negative rods, and because of synergy with penicillin agents against GBS as well as S. aureus, enterococci, and Listeria. S. aureus exhibits in vitro susceptibility but break-through colonies appear within 24 to 48 hours—therefore, gentamicin by itself has little activity against staphylococci and has to be combined synergistically with a beta-lactam agent. Hospital data from developing countries indicate that Gram-negative rods are increasingly resistant to gentamicin, but this needs to be confirmed in community settings. 57
What should the treating physician dictate?
The treating physician should dictate the frequency of office visits, giving consideration to patient characteristics, the nature of the infection, the patient’s tolerance of and response to therapy, and individual patient social factors. Antimicrobial Stewardship. XVII.
What is OPAT in medical terms?
Outpatient parenteral antimicrobial therapy (OPAT) is defined as the administration of parenteral antimicrobial therapy in at least 2 doses on different days without intervening hospitalization. Recommendations made in the updated guideline for the prescription and management of OPAT are summarized below. The panel followed a process used in the development of other Infectious Diseases Society of America (IDSA) guidelines, which included a systematic weighting of the strength of the recommendation and quality of evidence using Grading of Recommendations Assessment, Development and Evaluation (GRADE) (Figure 1) [2–5]. This revision focuses on systematically reviewing the literature to answer specific OPAT practice questions using published evidence. Readers are referred to the 2016 IDSA OPAT eHandbook for a more in-depth discussion of background and hands-on advice on the practice of OPAT [6]. Best practice tables that address pharmacokinetic features, administration options, and potential adverse effects of selected antimicrobials are included in this guideline. The guideline is not intended to replace clinical judgment in the management of individual patients. A detailed description of the methods, background, and evidence summaries that support each recommendation can be found online in the full text of the guideline.
Is debridement of necrotic tissue effective?
Additionally, treatment is always more effective if adequate source control is achieved, such as debridement of necrotic tissue, drainage of abscesses, and removal of infected prosthetic devices. Whenever possible, control at the primary site of infection should be addressed appropriately early in treatment.
Can you be hospitalized for parenteral antimicrobial therapy?
Currently in the United States, patients rarely remain hospitalized solely to complete a course of parenteral antimicrobial therapy. Except for some persons who inject drugs (PWID), most patients are eligible for some form of OPAT.
Is the guideline intended to replace clinical judgment in the management of individual patients?
The guideline is not intended to replace clinical judgment in the management of individual patients. A detailed description of the methods, background, and evidence summaries that support each recommendation can be found online in the full text of the guideline.
Can a nurse administer opat?
In traditional home-based infusion models in the United States, patients self-administer their OPAT medications and have a weekly visit by a visiting nurse. In other countries, OPAT at home may mean daily visits by an infusion nurse. In the TT model of home-based OPAT, there are no home visits by a nurse.
Why do we need antibiotics?
Antibiotics are only needed usually for prolonged or severe infections caused by bacteria when the body needs help to fight the infection. With some infections, intravenous antibiotics are more effective than oral antibiotics at treating the severity or type of infection that has occurred.
How long do you need to take antibiotics for a hip infection?
Some infections only require a short course of antibiotics (e.g. skin infections) but other infections may need treatment for many weeks (e.g. infection in a hip replacement). You will be informed how long you will need to receive intravenous antibiotics prior to commencing your treatment.
What is OPAT treatment?
Outpatient parenteral antibiotic therapy (OPAT) is mostly suitable for patients with skin infection or infections that require prolonged intravenous treatment such as infections in bone and joints or heart valves. To receive this treatment, it will be necessary for you to travel to Castle Hill Hospital either daily or three times a week.
How long does it take to get OPAT treatment?
Treatment times vary from 15 minutes to 2 hours depending on the type of antibiotic you require. In order to be considered for OPAT you will be referred to a Consultant in Infectious Diseases.
Can antibiotics cause discomfort?
This is because antibiotics may destroy your body’s harmless bacteria as well as the bacteria responsible for the infection you are being treated for. It can cause some discomfort but is easy to treat. If you are suffering from any of these side effects, please discuss them with the OPAT Specialist Nurse.
Can you drive to the OPAT clinic?
If you have not received any intravenous antibiotic treatment in hospital prior to attending the OPAT Clinic, it is strongly advised that you do not drive yourself to clinic or home following your first few treatments, until you know how your antibiotic therapy affects you.
Can antibiotics be changed?
bone infection), improvement can take much longer. Sometimes your doctor may change the type of antibiotic you are taking if they are concerned that it is not working, or if tests indicate this is necessary.
Parenteral Definition
The term parenteral in medical terminology means beyond the intestine (par = beyond, enteral = intestines). Thus, parenteral in medicine means the input of drugs or medications into the human body in a way not involving the intestines or the digestive tract.
Use of Parenteral Therapy
The administration of medications via parenteral therapy is very important in certain situations such as:
Parenteral Route
Parenteral medications are typically injected in four different ways depending on the layer of the skin that is the target of administration of the drug. There are 4 different layers where parenteral medication can be injected: epidermis, venous, subcutaneous, and intramuscular.