What is a DSAEK procedure?
DSAEK is a partial thickness cornea transplant procedure that involves selective removal of the patient's Descemet membrane and endothelium, followed by transplantation of donor corneal endothelium in addition to donor corneal stroma (Figure 8). The transplanted tissue is approximately 100-200 microns thick.
Is DSAEK or DMEK the best option for You?
DSAEK and DMEK are best suited for patients with conditions related to the endothelial cells, which include: A full-thickness corneal transplant will still be required for patients with corneal scarring or other conditions such as keratoconus. Are There Any Risks With DSAEK or DMEK Surgery?
What does DSAEK stand for?
Descemet Stripping Automated Endothelial Keratoplasty (DSAEK) DSAEK is a partial thickness cornea transplant procedure that involves selective removal of the patient's Descemet membrane and endothelium, followed by transplantation of donor corneal endothelium in addition to donor corneal stroma (Figure 8).
What are the leading indications for DSAEK?
First, diagnose. The leading indications for DSAEK are Fuchs dystrophy, pseudophakic corneal edema, failed corneal graft, and iridocorneal endothelial syndrome, said Allan R. Slomovic, MD, at the University of Toronto.

What is a Dsaek procedure?
Descemet's Stripping Automated Endothelial Keratoplasty (DSAEK) is a partial thickness corneal transplant. During this procedure, the patient's damaged endothelial layer is isolated and removed.
How successful is Dsaek surgery?
Overall success rate for primary DSAEK was 91.0%. After excluding the first 50 cases, success rate for primary DSAEK was 95.98%(n=195).
How long is Dsaek surgery?
DSAEK begins with only a small incision on the side of the cornea. The inner layer of the cornea is removed and a donor layer is put in to place. The entire procedure takes approximately one hour.
What is the difference between DMEK and Dsaek surgery?
DMEK is very similar to DSAEK, with the primary difference being that the donor tissue implanted does not include any stromal tissue, but is instead a pure replacement of endothelium. A DMEK graft, therefore, is much thinner than a DSAEK graft.
How soon can I drive after a corneal transplant?
You must not drive on the day of your cornea transplant. Someone must drive you home after surgery and bring you back for your follow-up visit. If you have good vision in the non-transplant eye, you can legally drive 24 hours after surgery. However, your surgeon may recommend waiting longer before driving.
How long do stitches stay in after corneal transplant?
After six months, the wound is considered effectively closed, and all sutures can be removed. If the patient is happy with their vision, sutures could even be left in place indefinitely but should be removed in case of loosening, breaking, inflammation, infection, or vascularization.
What is the difference between DSEK and Dsaek?
DSEK involves a transplant of the back layers of a donor cornea into a patient's eye. DSAEK is the automated version of this procedure, which uses a machine to cut tissue.
Do you go blind with Fuchs dystrophy?
Without a corneal transplant, a person with severe Fuchs dystrophy may become blind or have severe pain and very reduced vision. Mild cases of Fuchs dystrophy often worsen after cataract surgery.
How painful is a corneal transplant?
Are cornea transplants painful? The cornea transplant procedure itself is not painful. Your surgeon will use a local anesthetic to numb your eye and may give you general anesthesia or a sedative if you're feeling anxious about the transplant.
Which is better DMEK or Dsaek?
Despite DSAEK standing out as the easier technique, there are other factors to consider. DSAEK is often preferred to DMEK because primary failure is more common with DMEK, Dr. Busin said. He said DMEK poses the threat of a significant detachment rate.
What is one disadvantage of DMEK over Dsaek?
DMEK may be associated with more early surgical complications. Graft dislocation may happen in one or two out of 100 people with DSAEK and about five times more often with DMEK.
How long does DMEK last?
As the gas bubble dissipates over seven to ten days, vision continues to improve. When there are no other eye problems, DMEK can result in 20/20 vision within a few months after treatment.
How long does a DSEK transplant last?
Late failure of the graft is certainly possible, but as mentioned earlier most grafts are expected to last at least 20 to 30 years, and they can be replaced if necessary. The air bubble may cause an increase in pressure inside the eye.
How long is recovery from DMEK surgery?
Patients may be able to resume driving and performing light activities within a week after DMEK surgery. Eighty percent of the healing that needs to occur takes place within the first month after treatment. Full recovery is usually complete within four to six months.
What is the difference between DSEK and Dsaek?
DSEK involves a transplant of the back layers of a donor cornea into a patient's eye. DSAEK is the automated version of this procedure, which uses a machine to cut tissue.
How does cornea transplant work?
During a full-thickness cornea transplant (penetrating keratoplasty), a circular disk-shaped portion of your cornea is removed and replaced with a similarly sized portion of cornea from a donor. A cornea transplant (keratoplasty) is a surgical procedure to replace part of your cornea with corneal tissue from a donor.
What is a DSEK?
Descemet’s stripping endothelial keratoplasty (DSEK) replaces diseased tissue with a thin donor graft of posterior corneal stroma, Descemet’s membrane, and endothelium. In DSAEK, use of an automated microkeratome facilitates donor preparation and reproducible results. 1 This review covers the main steps of DSAEK, from patient selection to postop care.
What to look for before DSAEK?
Screen for risks. Before DSAEK, look for conditions that may predispose patients to complications during surgery, said Mark J. Mannis, MD, with the University of California, Davis, Health System Eye Center. Ensure that the eye is stable and free of active macular edema or elevated intraocular pressure, said Dr. Suh, who noted some conditions that may make the procedure more challenging, yet still possible: a shallow anterior chamber (more common in smaller eyes), glaucoma, presence of a filtering bleb or tube, presence of an anterior chamber lens, absence of a portion of the iris, floppy iris syndrome, or aphakia. (See “ Tips for Higher-Risk Cases .”)
What is the mark used to cut a DSAEK donor?
Mark the epithelium. Using a circular trephine of the same size used to cut the DSAEK donor, Dr. Slomovic makes an impression on the recipient’s corneal epithelium, indicating the area of Descemet’s membrane that will be removed.
What forceps do they use for a donor disc?
Specialized forceps. Dr. Slomovic uses either Busin forceps or Tan forceps to pull the donor disc into the anterior chamber through a paracentesis that is 180 degrees away from the donor insertion point. These forceps have been designed to minimize crush injuries, he said.
How to score Descemet's membrane?
1. Score Descemet’s membrane 360 degrees at a diameter of about 8.5 mm with a reverse Sinskey hook, using the epithelial trephine groove as a guide. 2. Detach the tissue in a circular fashion, taking care not to use excessive force, which can irritate the stroma. 3.
How to do descemetorhexis?
Mannis, who generally uses a retrobulbar block instead to immobilize the eye and keep the patient completely pain free. The first step involves making a peripheral side-port incision (paracentesis), through which an anterior chamber (AC) maintainer is placed to keep the anterior chamber formed, said Dr. Slomovic. Surgeons will perform the descemetorhexis using either an AC maintainer or, especially if the procedure is combined with cataract surgery, cohesive viscoelastic. (See “ Combination Surgery: Cataract and DSAEK .”)
Can eye banks cut DSAEK?
Initially, few U.S. eye banks provided precut DSAEK tissue, said Dr. Mannis, but today it’s more common than not, reducing the ophthalmologist’s surgical time and need for capital equipment. “The literature also demonstrates that DSAEK tissue cut by eye bank technicians is just as effective as that harvested by a doctor,” he said.
What Is DSAEK/DMEK (Partial Thickness Corneal Transplant) Surgery?
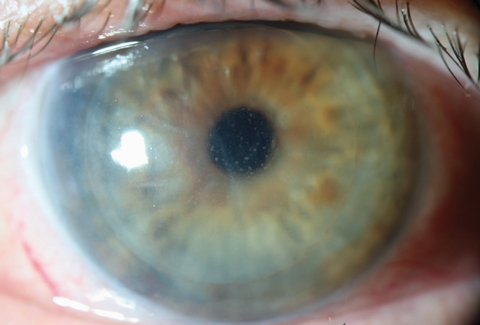
The cornea is the clear dome at the very front part of the eye and is composed of five main layers. The endothelium is a single layer of cells coating the inside portion of the cornea. While the endothelium has many functions, one of its most important functions is to serve as a layer of vacuum pumps in order to pump fluid out of the cornea and keep it crystal clear. If the endothelium malfunctions, excess fluid can build up in the middle layers of the cornea and cause swelling of the cornea (corneal edema), leading to decreased vision. Patients report this blurry vision as “looking through a foggy shower door”. Some patients (such as those with Fuchs endothelial dystrophy) report this foggy vision is worst immediately after waking up in the morning and gets slightly better as the day goes on. Other patients with corneal edema due to other causes report blurry vision that is constantly poor throughout the day.
What is DMEK best suited for?
DSAEK and DMEK are best suited for patients with conditions related to the endothelial cells, which include:
What is a DMEK?
Descemet’s stripping automated endothelial keratoplasty (DSAEK) and Descemet’s membrane endothelial keratoplasty (DMEK) are partial thickness corneal transplants performed to replace the endothelium (the innermost portion of the cornea). DMEK is very similar to DSAEK, with the primary difference being that the donor tissue implanted does not include any stromal tissue, but is instead a pure replacement of endothelium. A DMEK graft, therefore, is much thinner than a DSAEK graft.
What is the rejection rate for DMEK?
The rejection rate for DSAEK patients is about 10% while for DMEK patients it is less than 1%.
Is DMEK the same as DSAEK?
DMEK is very similar to DSAEK, with the primary difference being that the donor tissue implanted does not include any stromal tissue, but is instead a pure replacement of endothelium. A DMEK graft, therefore, is much thinner than a DSAEK graft.
Are There Any Risks With DSAEK or DMEK Surgery?
With both DSAEK and DMEK, there are normal risks associated with eye surgery such as infection, bleeding, and swelling ( your surgeon will discuss the risks in more detail), but there are also the risks of rejection and displacement.
What is DSEK corneal surgery?
DSEK is intended to transplant a healthy endothelial cell layer that will pump the fluid out of the cornea. It’s expected to restore corneal clarity and improve vision. This procedure corrects corneal endothelium failure, but is not able to correct corneal scarring, thinning or surface irregularity.
What antibiotics should be given after DSEK?
Postoperative care should include broad-spectrum antibiotics to prevent infection and steroids (initially dexamethasone, then fluorometholone) to prevent rejection. Patient should lie in the supine position for one more day after DSEK (to utilize the residual air bubble in the anterior chamber) and to not rub their eye for 2 weeks after DSEK surgery.
How to graft a descemetorhexis?
Surgical technique: With a reverse Sinskey hook, a circular portion of Descemet membrane is scored and stripped from the posterior stroma so a descemetorhexis is created and the central portion of Descemet membrane is removed from the eye. A temporal self-sealing 5.0 mm sclerocorneal incision is created with a crescent knife. After trephinating an 7.5 to 9.0 mm diameter DSEK-graft from the predissected corneoscleral rim, the tissue is often stained with Trypan Blue. The graft can be inserted with a wide variety of techniques. Irrigating inserters, push-through and pull through techniques exist. Irrigating inserters rely on the adhesion between the insertion platform and the posterior stromal surface as the insertion platform gently springs open in the anterior chamber. Push-through techniques rely on forceps, hooks bent-needles and glides to slide a graft into the anterior chamber, usually on a film of viscoelastic. Pull-through techniques is a two-handed maneuver employing specialized forceps or suture position on the opposite side of the main wound to draw the donor disc into the anterior chamber, with or without a glide. Finally, a manual folding forceps insertion technique requires the surgeon to fold the graft in a 60%/40% ratio, like a taco, and carefully insert and rotate the graft to the appropriate position. . If a glide is used for insertion, it is removed from the main wound, and the DSEK graft is unfolded in the recipient anterior chamber, taking care to avoid excessive touch between the donor endothelium and the underlying iris and lens. Balanced salt solution, an air bubble, or instrument manipulation may be used to assist in the unfolding of the graft. After unfolding, the graft is positioned against the posterior stroma of the host using a small air bubble. The DSEK graft is then carefully positioned centrally using a variety of brushing, tapping , sweeping and dragging techniques. After the DSEK graft is positioned centrally, the anterior chamber is completely filled with air. . Dilating drops may be used to prevent any pupillary block from air bubble. Peripheral iridotomies can also be performed to reduce the chance of pupillary block. Once the donor disc is in tight apposition with no or minimal interface fluid between the donor and the recipient stroma, the surgeon partially removes the air in the anterior chamber and replaces it with BSS. An air bubble of approximately 8 to 9 mm is usually left in place to help further stabilize the donor disc position over the first 24 hours postoperatively. The air bubble pushes the graft in place until it heals in an appropriate position, giving time for the pumping action of endothelium to help the donor tissue bind to its new host . The structure of the cornea remains intact.
What is EK in medical terms?
Endothelial Keratoplasty (EK) has been adapted as an alternative in the treatment of corneal endothelial disorders. In the various forms of endokeratoplasty, Descemet’s membrane and the endothelium are replaced, with or without a varying amount of corneal stroma. In Descemet’s stripping endothelial keratoplasty (DSEK), ...
How long does it take for a DSEK transplant to be rejected?
Graft Rejection: Rejection can develop months or years after the transplant. Against PK, initial rejection symptoms after DSEK procedure are usually subtle. Patients can be asymptomatic. When patients show redness, blurry vision and light sensitivity the rejection is severe. To prevent rejection patients should be under a closed follow-up care and kept on a prophylactic tapering down eye drop steroids regimen.
How are corneoscleral buttons excised?
Donor tissue preparation: Corneoscleral buttons are excised from donor globes and stored by organ culture. Each globe is mounted on a purpose-designed holder and the anterior chamber is filled with air to create an air-endothelium interface. With dissection spatulas, a manual stromal dissection is made at approximately 95% stromal depth using air-to-endothelium reflex to monitor dissection depth. Stromal dissection is extended up to limbus over 360 degrees. After dissection is completed, a 16.0 mm corneoscleral rim is excised from each globe and the endothelium is evaluated with an inverted light microscope and stored in organ culture until time of transplantation.
How long does it take to remove a donor cornea?
Surgical Technique. This procedure, which takes approximately 45 min, is done under local or general anesthesia. First the endothelium and Descemet’s membrane of the cornea is stripped away through a corneal incision. Then a circular disc is removed from the inner lining of a donor cornea.
What is DSAEK in medical terms?
Video 3: Descemet stripping automated endothelial keratoplasty (DSAEK) is an endothelial replacement procedure in which dysfunctional corneal endothelium is replaced with a graft consisting of donor endothelium and a thin layer of posterior stroma to facilitate handling of the tissue. This case was performed for severe corneal edema secondary to pseudophakic bullous keratopathy. Contributed by Jesse Vislisel, MD, and Mark A. Greiner, MD
How thick is a DSAEK cornea?
DSAEK is a partial thickness cornea transplant procedure that involves selective removal of the patient's Descemet membrane and endothelium, followed by transplantation of donor corneal endothelium in addition to donor corneal stroma (Figure 8). The transplanted tissue is approximately 100-200 microns thick. If the endothelium of the graft makes contact with any surgical instruments, it will be damaged and the graft may fail; therefore, the surgical procedure is designed to avoid contacting the donor endothelium. A tunneled corneoscleral incision is created, the recipient endothelium and Descemet membrane is removed, the graft is folded and inserted with non-coapting forceps (forceps that do not meet at the tips), and an air bubble is placed in the anterior chamber to support graft adherence. The procedure is used to treat corneal edema in the setting of endothelial dystrophies (such as Fuchs corneal dystrophy and posterior polymorphous corneal dystrophy ), pseudophakic bullous keratopathy, iridocorneal endothelial (ICE) syndrome, endothelial failure in the setting of prior intraocular surgery or of a previous PK graft, and other causes of corneal endothelial dysfunction ( 1, 17-20 ).
What eye drops are used after DMEK/DSAEK surgery?
You will need to use an anti-inflammatory steroid (dexamethasone) and antibiotic drops (moxifloxicin or chloramphenicol) after surgery. In some cases you may be asked to use sodium chloride drops (salt drops) to aid corneal clearance.
What should you watch out for after DMEK/DSAEK surgery?
However, if you experience severe pressure like pain in the 24 hours after your surgery you should contact your doctor or the hospital. If this is accompanied by loss of perception of light (everything is dark and you can’t see light shone on the eye) you should seek urgent attention as this can be an indication of dangerously raised pressure in the eye. The walk-in eye emergency clinic is open at Moorfields 24 hours a day every day of the year and you will be seen at any time if you are worried.
How long does it take for DMEK to heal?
The new cell layer is held in place by an air/gas bubble that supports the new layer and gradually disappears over 3-5 days. Unlike a full thickness corneal transplant, very few stitches are used in DMEK/DSAEK surgery and visual recovery is more rapid. Rejection rates are also lower after these surgeries.
What is the phone number for DMEK?
If you have questions about DMEK/DSAEK surgery and the options that are available for you, please call us on 0203 369 2020, or request a call back. DMEK and DSAEK are both advanced surgeries for Fuchs’ dystrophy and other causes of corneal endothelial failure, during which a very thin layer of new cells is placed inside the eye.
What to expect in the first 5 days after DMEK surgery?
What to expect in the first 5 days after DMEK/DSAEK surgery. The front chamber of the eye will be filled with gas/air and hence vision will be impaired. It is not possible to see through an air bubble in the eye. Vision will typically be worse than before the surgery. You will be able to see light and blurred shapes.
How long does it take for vision to improve after DMEK?
Visual recovery after DMEK/DSAEK takes 1-4 weeks. Typically vision is poor in the first few days due to the air bubble. Vision begins to improve once the bubble is above the level of the pupil. Good vision can be expected a month after surgery. New glasses can typically be measured 6 weeks after surgery.
How long after DMEK can you get air?
Further air injection after DMEK/DSAEK. Your surgeon will typically review your eye 3-5 days after surgery. At this stage, if there is any part of the graft that is not attached the surgeon may choose to inject further air into the eye.
What are the advantages of DSAEK?
Steven I. Rosenfeld, MD, a cornea surgeon in private practice in Delray Beach, Fla., cited the main advantages of DSAEK as: 1 a faster surgery, 2 quicker visual recovery, 3 less intraoperative risk and 4 less postoperative irritation and astigmatism.
What are the complications of DSAEK?
In addition to dislocation and failure, complications extending to other ocular structures are a potential DSAEK risk. These include retinal detachment, cystoid macular edema, suprachoroidal hemorrhage, steroid-response glaucoma, pupillary block from the injected air bubble and IOL dislocation. “This is what we know so far, but we are still learning,” Dr. Rosenfeld noted. “When DSAEK first came out, many of these complications hadn’t been reported yet or hadn’t been fully recognized. Now we are realizing that this surgery—as good as we think it is—is still prone to the complications that you can see in many types of intraocular surgery.”
How many cases of DSAEK are comfortable?
Regarding learning curves, Dr. Rosenfeld said, “In my opinion, it takes about 10 cases to start feeling comfortable with DSAEK and about 50 cases to feel fully comfortable. But I can say that when you get together with other cornea surgeons who do DSAEK, we all still find it very humbling. On face value it looks like a rather simple, straightforward operation, but the infinite number of ways you can have little glitches during surgery never ceases to amaze us, and we are still learning how to handle them.”
Why is DSAEK vulnerable to dislocation?
Dislocations. Corneal transplants performed with DSAEK are vulnerable to dislocations because the donor tissue is held in place with an air bubble instead of sutures. After the donor tissue is placed against the host cornea, an air bubble is injected into the eye and presses against the graft to keep it in place.
Is Descemet a mainstream procedure?
In the last five years, refinements in Descemet’s stripping automated endothelial keratoplasty (DSAEK) have moved the procedure from experimental status to mainstream use. According to Mark S. Gorovoy, MD, a cornea surgeon in private practice in Fort Myers, Fla., and an early proponent of DSAEK, these grafts now account for at least half of the corneal transplants performed in the United States today.
Is DSAEK better than PK?
DSAEK has several advantages over conventional penetrating keratoplasty (PK). But the procedure also has a significant learning curve and several potential complications that have come to light as more DSAEK transplants are being performed. These complications are generally manageable, and the risk tends to decline as a surgeon gains experience in the new surgical technique.
What is DSEK procedure?
With a DSEK procedure, only the abnormal inner lining of the cornea is removed. A thin, circular disc is then removed from the inner lining of a donor cornea. This is folded and placed inside of the eye where an air bubble pushes it in place until it heals in an appropriate position. No sutures are required and the structure of the cornea remains intact, leading to a faster visual recovery and less astigmatism.
What is DSEK surgery?
Descemet’s Stripping with Endothelial Keratoplasty (DSEK) a newer cornea transplant technique that replaces only the damaged cell layer instead of replacing the entire thickness of the cornea. With this technique, the cornea heals much faster and stronger and the patient’s visual recovery is better. Because this technique leaves a smoother surface and significantly improves the visual results, it has become a preferred method for treatment for Fuchs’ Dystrophy and pseudophakic bullous keratopathy. If you’re interested in DSEK Eye Surgery, schedule an appointment at the Cleveland Eye Clinic and speak with our doctors to get all your questions answered.
How long does it take to get a DSEK?
The DSEK procedure is done under local anesthesia and takes approximately 45 minutes. For the first 24 hours after surgery, you will be asked to lie on your back with your face pointed directly to the ceiling for as much time as you can tolerate.
What is a PKP cornea?
Penetrating Keratoplasty (PKP) involves replacing an eye ’s scarred, diseased, or damaged cornea with clear corneal donor tissue. This procedure can improve visual acuity as it is replacing the cloudy cornea with clear donor tissue. PKP is suitable for those with corneal decomposition, corneal dystrophies (other than keratoconus) including Fuch’s Dystrophy, and corneal trauma/corneal scarring.
What size incision is used for DSAEK?
During bifold forceps insertion, the incision size is important, because trauma to the endothelium may occur if the incision is too small. Because of this concern, a 5-mm incision is recommended in DSAEK. The same incision size is used with the Busin glide to prevent compression of the tissue and secondary loss of endothelium. With cartridge injector suture pull-through techniques, a 3.5- to 4-mm clear corneal incision may be used, and endothelial cell loss is similar to that seen with bifold forceps insertion in DSAEK. 3
How thick is DSAEK tissue?
At the present time, there is a trend toward the use of ultra-thin DSAEK tissue, which has a thickness of 50 to 75 µm, rather than the traditional 100 to 200 µm. Ultra-thin DSAEK donors probably do provide a faster recovery and allow the surgeon to use newer, small incision insertion devices, since thinner tissue is less likely to become damaged from compression. However, in terms of complications, ultra-thin grafts may have a higher risk of postoperative striae that could impair vision and are more difficult to handle during and after insertion (especially for the inexperienced DSAEK surgeon). It should be noted that microstriae after DSAEK often improve with time, although macrostriae usually will require disc replacement.
How big of a graft should I use for DSAEK?
In patients with large corneal diameters or an increased anterior chamber depth, an increase in diameter to 8.5 to 9.5 mm may be appropriate, however I rarely use graft diameters in this range. In special cases such as buphthalmia or high myopia, though, an increase in diameter to 9.5 mm is common in my practice. In general, smaller diameter DSAEK buttons are associated with fewer complications, because the insertion is easier, less air is needed for adhesion, and there is a decreased chance of PAS formation. For these reasons, I recommend that the beginning DSAEK surgeon use grafts that are 8 to 8.25 mm in diameter. Then, with experience, larger diameter buttons can be used more reliably. Keep in mind that current research at Devers Eye Institute in Portland, Ore., has clearly shown that DSAEK with a graft diameter of 8.5 mm does not offer a clinical advantage over smaller 8-mm grafts, with respect to postoperative endothelial cell counts at two years after surgery. 1
What size DSAEK button should I use?
For these reasons, I recommend that the beginning DSAEK surgeon use grafts that are 8 to 8.25 mm in diameter.
Why is a 5mm incision needed for DSAEK?
During bifold forceps insertion, the incision size is important, because trauma to the endothelium may occur if the incision is too small. Because of this concern, a 5-mm incision is recommended in DSAEK. The same incision size is used with the Busin glide to prevent compression of the tissue and secondary loss of endothelium.
Why do you need a PK button for endothelial graft?
In both situations, if the endothelial graft and the recipient cornea show infiltration, a PK will be required to ensure that the infection is eradicated. If only the endothelial graft is affected, removal of the DSAEK button is the logical choice.
Patient Selection
- Indications
Not all patients with corneal pathology are candidates for DSEK. The indication depends on decreased vision related to corneal swelling from poorly functioning endothelium. The main indications are: 1. AcquiredPseudophakic or Aphakic bullous keratopathy, Failed previous graft. …
Surgical Technique
- This procedure, which takes approximately 45 min, is done under local or general anesthesia. First the endothelium and Descemet’s membrane of the cornea is stripped away through a corneal incision. Thena circular disc is removed from the inner lining of a donor cornea. This thin layer is then transplanted into the recipient eye and attached to the posterior cornea of the recipient. Do…
Advantages and Challenges
- DSEK Procedure Advantages
Over PK: 1. Less Invasive, smaller surgical incisions 2. No corneal-graft sutures 3. Faster visual recovery 4. Less risk of sight threating complications and less induced astigmatism 5. Post-surgery stronger eye (less prone to injury) 6. Less risk of immune rejection of the transplanted c… - DSEK Procedure Challenges
Compared with DMEK: 1. Final Best Corrected Visual Acuity (BCVA) may be suboptimal . Optical irregularities due to stromal layers being transplanted in DSEK. For nano-thin DSEK, final BCVA was comparable to DMEK, demonstrating the significance of thinner donor graft preparation. 2. …
Follow Up Care
- Slit lamp biomicroscopy:to ensure that the graft is fully attached and to look for signs of rejection (scattered keratic precipitates, edema or conjunctival hyperemia). Fig. 1.
- Check IOP:monitor for steroid-induced pressure spikes.
- Check refractionafter first month.
- Check central corneal thickness:a graft that is getting thicker over time may be failing and a …
- Slit lamp biomicroscopy:to ensure that the graft is fully attached and to look for signs of rejection (scattered keratic precipitates, edema or conjunctival hyperemia). Fig. 1.
- Check IOP:monitor for steroid-induced pressure spikes.
- Check refractionafter first month.
- Check central corneal thickness:a graft that is getting thicker over time may be failing and a graft that gets thicker suddenly signals rejection.
Conclusion
- Even though DSEK/DSAEK may be the current standard, the newer partial thickness Descemet’s Membrane Endothelial Keratoplasty may have better clinical outcomes and may also require less investment in preparation of isolated Descemet grafts. A study compared outcomes after DMEK and DSEK during the surgeon’s DMEK learning curve and there was some evidence of improved …
Additional Resources
- Boyd K, DeAngelis KD. Iridocorneal Endothelial Syndrome . American Academy of Ophthalmology. EyeSmart® Eye health. https://www.aao.org/eye-health/diseases/iridocorneal-endothelial-syndrome-5. Acces...