How long should you give a PD-1 inhibitor?
The Dosage and Administration section of labeling for all five currently approved PD-1/PD-L1 inhibitors recommends giving drug until disease progression or unacceptable toxicity. In addition, labeling for Merck & Co. Inc.'s PD-1 inhibitor Keytruda (pembrolizumab) advises dosing for up to 24 months in patients without disease progression.
How does PD-1 overexpress on tumor cells?
For example, PD-L1, as the ligand of PD-1, could overexpress on tumor cells to evade the antitumor immune response by repressing the activation and function of CD8+T cells ( 1 ). Anti-PD-1 is one of the most promising attractive anticancer immune checkpoint blockers (ICB).
What happens when PD-L1 binds to PD-1?
Generally, when PD-L1 binds to PD-1 in the presence of the T cell receptor (TCR) signaling complex, PD-1 delivers a co-inhibitory signal, leading to the termination of TCR signaling and inhibition of T cell proliferation ( 11 ).
Is pd-1-blocking therapy less effective when there is no target mutation?
It means that the PD-1-blocking therapy may be less effective if the tumor does not contain a mutation that can be a target. Despite the underlying mechanism being still unclear, evidence highlights that the combination of radiotherapy (RT) and anti-PD-1 is considered a promising strategy ( 132 ).

Can you rechallenge with PD-L1 inhibitors after progression?
There are some emerging reports about rechallenging with PD-1/PD-P1 inhibitors in patients who were previously treated with anti-PD-1 or anti-PD-L1 and discontinued treatment with these agents for disease progression. It was first reported by Lipson et al.
Do cancer cells express PD-1?
PD-1 is mainly expressed on the activated T cells, B cells, and monocytes (31). Recent studies have shown that PD-1 is expressed in a subpopulation of various cancer cells, including melanoma (23), hepatocellular carcinoma (HCC) (32), and NSCLC (22).
Is PD-L1 positive good?
PD-L1 positivity is only desirable in the context of treatment targeting the PD-1–PD-L1 interaction, as in the absence of this therapy it may be a mechanisms of immune escape that is only beneficial to the cancer cells.
What happens when PD-L1 binds to PD-1?
The binding of PD-L1 to PD-1 on T cells results in the dephosphorylation of the T-cell receptor (SHP-1/2). It inhibits T cells from killing cancer cells by reducing T cell proliferation and activity4.
How does PD-1 enable tumors to grow?
The interaction of PD-L1 on cancer cells with PD1 on the surface of T-cells causes cancer cells to escape from the immune system by preventing the activation of new cytotoxic T-cells in the lymph nodes and subsequent recruitment to the tumor.
Do all cancer cells have PD-L1?
Some cancer cells have high amounts of PDL1. This allows the cancer cells to "trick" the immune system, and avoid being attacked as foreign, harmful substances. If your cancer cells have a high amount of PDL1, you may benefit from a treatment called immunotherapy.
What is considered a high level of PD-L1?
A PD-L1 test measures what percentage of cells in a tumor “express” PD-L1. Tumors that express high amounts of PD-L1 (50% or greater) may respond particularly well to checkpoint inhibitors (a type of immunotherapy drug). If you have not had your PD-L1 levels tested, ask your doctor if it is right for you.
What is a good PD-L1 score?
Although the result of the CPS calculation can exceed 100, the maximum score is defined as CPS 100. A minimum of 100 viable tumor cells in the PD-L1–stained slide is required for the specimen to be considered adequate for PD-L1 evaluation.
What percentage of PD-L1 is positive?
PD-L1 positivity prevalence of 1% and 50% cut-off was 43.4% and 16.6%, respectively, but was significantly more frequent in higher stages. PD-L1 positivity was associated with better prognosis for non-metastatic NSCLC patients and for adenocarcinoma patients, but no effect was found for the squamous cell carcinoma.
Can PD-L1 change over time?
Abstract. Background/aims: Programmed death-ligand 1 (PD-L1) expression, a validated predictive biomarker for anti-PD-1/PD-L1 inhibitors, is reported to change over time. This poses challenges during clinical application in non-small cell lung cancer.
How does PD-L1 therapy work?
When PD-1 binds to PD-L1, it basically tells the T cell to leave the other cell alone. Some cancer cells have large amounts of PD-L1, which helps them hide from an immune attack. Monoclonal antibodies that target either PD-1 or PD-L1 can block this binding and boost the immune response against cancer cells.
Is PD-L1 on healthy cells?
PD-L1 may be found on some normal cells and in higher-than-normal amounts on some types of cancer cells.
Background
Immune surveillance functions of innate and adaptive immune cells can be suppressed by multiple mechanisms in the tumor microenvironment (TME); the most noted one is the programmed cell death receptor 1 (PD-1)/programmed cell death ligand 1 (PD-L1) pathway.
The Role of PD-1 and PD-1 Inhibitors in Immune Response
PD-1, a member of the B7-CD28 receptor family, is a transmembrane protein and widely expressed in B cells, T cells, natural killer (NK) cells, and myeloid cells ( 7 ). As the ligand of PD-1, programmed cell death ligand 1 (PD-L1) can be expressed in dendritic cells (DCs), macrophages, T cells, NK cells ( 8, 9 ), and tumor cells ( 10 ).
Immune Microenvironment
Immunotherapies based on PD-L1/PD-1 blockade have revolutionized the treatment paradigm for several cancer types. Their interaction regulates the activation of immune responses and specifically of T cell responses in physiological conditions.
TAMs
TAMs are major components of infiltrated leukocytes in tumors, which dominantly orchestrate cancer-related inflammation ( 115 ). They can be divided into two subtypes: M1 and M2. Anti-tumorigenic M1 macrophages express high levels of TNFα, inducible nitric oxide synthase (iNOS), and MHC class II molecules.
Drug Resistance and Combined Therapy
Anti-PD-1 therapy has shown significant efficacy in clinical trials and has been approved for treating several cancers in clinic therapy. However, the occurrence of primary or acquired drug resistance will cause the patient to be ineffective to PD-1 blockade therapy or eventually the recurrence of malignant tumors ( 127 ).
Conclusions
In this review, we primarily describe a complex story of the relationship between anti-PD-1 and TME. The initiation of the antitumor effect depends on the cross talk between immune cells ( Figure 1 ).
Author Contributions
QW wrote the manuscript; all authors were involved in the amendments and improvements in the text. All authors contributed to the article and approved the submitted version.
What is the effect of PD-1 on T cells?
In the cancer disease state, the interaction of PD-L1 on the tumor cells with PD-1 on a T-cell reduces T-cell function signals to prevent the immune system from attacking the tumor cells. Use of an inhibitor that blocks the interaction of PD-L1 with the PD-1 receptor can prevent the cancer from evading the immune system in this way. Several PD-1 and PD-L1 inhibitors are being trialled within the clinic for use in advanced melanoma, non-small cell lung cancer, renal cell carcinoma, bladder cancer and Hodgkin lymphoma, amongst other cancer types.
What is PD-1 inhibitor?
PD-1 inhibitors and PD-L1 inhibitors are a group of checkpoint inhibitor anticancer drugs that block the activity of PD-1 and PDL1 immune checkpoint proteins present on the surface of cells. Immune checkpoint inhibitors are emerging as a front-line treatment for several types of cancer. PD-1 and PD-L1 inhibitors act to inhibit the association ...
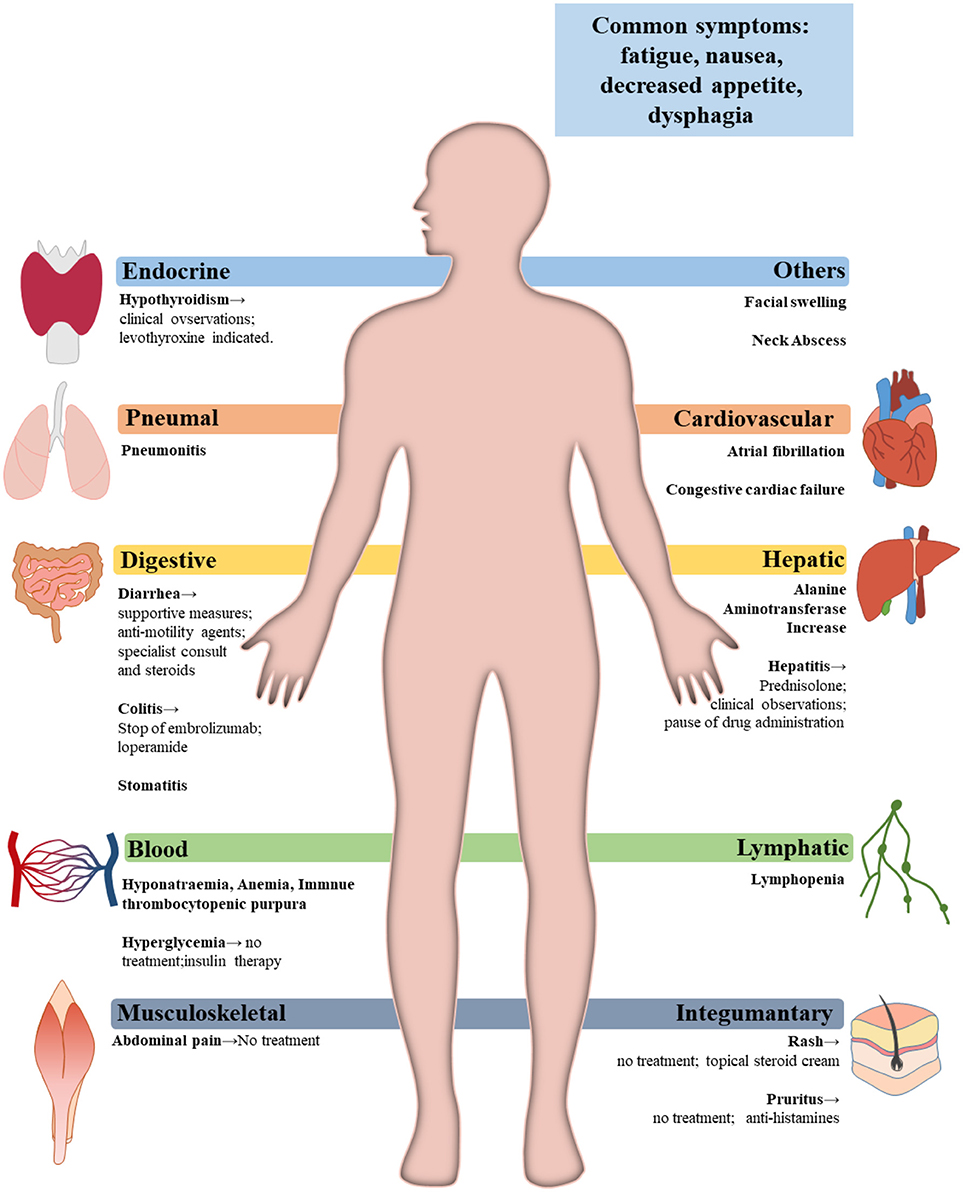
What are the effects of immunotherapy?
Some of these include interstitial pneumonitis, colitis, hepatitis, thyroiditis, skin reactions, low levels of platelets and white blood cells, inflammation of the brain or spinal cord, neuromuscular adverse events including myositis, Guillain-Barré syndrome, myasthenia gravis; myocarditis and cardiac insufficiency, acute adrenal insufficiency, and nephritis. The most common kidney related changes are acute interstitial nephritis, followed by glomerular diseases and then tubular damage. The detailed mechanism of these adverse effects are not fully elucidated; however, they are clearly different from known autoimmune diseases. Immune-mediated adverse reactions are usually attributed to generalised dysregulation of T cells or development of autoantibodies, although memory T cell responses against occult viral infections might also play a role in some patients with advanced melanoma following combined PD-1/CTLA-4 blockade.
What is the only PD-L1 antibody?
At least two PD-L1 inhibitors are in the experimental phase of development. KN035 is the only PD-L1 antibody with subcutaneous formulation currently under clinical evaluations in the US, China, and Japan. CK-301 by Checkpoint Therapeutics.
How many patients have PD-1 inhibitors been tested?
As of 2017, more than 500 clinical trials involving PD-1 and PD-L1 inhibitors have been conducted in more than 20,000 patients. By the end of 2017, PD-1/PD-L1 inhibitors had been approved for the treatment of nine forms of cancer.
When was PD-1 approved?
PD-1. Pembrolizumab (formerly MK-3475 or lambrolizumab, Keytruda) was developed by Merck and first approved by the Food and Drug Administration in 2014 for the treatment of melanoma. It was later approved for metastatic non-small cell lung cancer and head and neck squamous cell carcinoma.
When was PD-1 first used?
The concept of blocking PD-1 and PD-L1 for the treatment of cancer was first published in 2001. Pharmaceutical companies began attempting to develop drugs to block these molecules, and the first clinical trial was launched in 2006, evaluating nivolumab. As of 2017, more than 500 clinical trials involving PD-1 and PD-L1 inhibitors have been ...
What is PD-1 in melanoma?
Monotherapy with immune checkpoint inhibitors, specifically those targeting programmed death 1 (PD-1), has revolutionized the treatment of metastatic melanoma: approximately 40% of patients achieve a partial or complete response, many of which are durable. However, a subset of patients who initially respond to therapy will progress, ...
What is immune checkpoint blockade?
The use of immune checkpoint blockade has revolutionized the treatment of metastatic melanoma, with dramatic improvements in cancer-related outcomes since the advent of these agents. Long-term survival data demonstrate durable disease control in 20% and 30% of patients receiving the cytotoxic T-lymphocyte–associated antigen 4 (CTLA-4) antagonist ipilimumab and the programmed death 1 (PD-1) inhibitor pembrolizumab, respectively. [1,2] However, a subset of patients-approximately 40% to 45%-experience no response to therapy, with clear de novo resistance (primary resistance). The reasons for primary resistance include inadequate T-cell infiltration into the tumor, as well as immunosuppressive factors within the tumor microenvironment. [3,4] Treatment strategies to overcome these obstacles range from adoptive T-cell therapy to stimulate tumor antigen–specific T cells, to mitogen-activated protein kinase (MAPK) inhibition to improve T-cell trafficking into the tumor. [5]
Is immunotherapy a treatment for unresectable melanoma?
Immunotherapy has changed the treatment landscape for unresectable melanoma. However, despite the successes of front-line immune checkpoint inhibitor therapy, most patients will eventually progress. Post-progression treatment decisions should be made based on the site of progression, extent of disease progression, and clinical status of the patient. In the setting of oligometastatic progression, employment of local therapy with surgical resection or ablative radiotherapy is often preferred with continuation of immune checkpoint inhibitors. In contrast, transition to an alternative standard or investigational systemic agent (s) is required in cases of diffuse progression. The decision regarding next-line therapy requires assessment of both cancer- and patient-specific factors, such as the molecular features of the tumor (eg, BRAF mutation status), the performance status of the patient, and clinical trial availability. Advancements in translational biomarker research are crucial in order to refine this treatment algorithm. Pre- and on-treatment biomarker discovery will hopefully aid clinicians in identifying patients who are likely to respond to front-line monotherapy with immune checkpoint inhibitors; importantly, it will also help to provide further insights into the optimal therapeutic strategies for individuals with primary resistance and those destined to develop acquired resistance.
Is NKTR-214 a pro-drug?
However, severe toxicities, coupled with potential immunosuppressive effects, [67] have limited its use. NKTR-214, a pro-drug of IL-2, has subsequently been developed to generate the immune stimulatory benefits of the IL-2 pathway to maximize antitumor responses and minimize adverse effects. [68] .
Can PD-1 be used after progression?
Prior to transitioning to an alternative treatment approach, clinicians can consider continuing the use of PD-1 inhibitors after progression occurs. Whereas disease progression on chemotherapies and tyrosine kinase inhibitors (TKIs) almost uniformly results in treatment discontinuation due to futility of continued therapy, studies demonstrate the possibility of atypical and delayed response with immune checkpoint inhibitor therapy beyond Response Evaluation Criteria in Solid Tumors (RECIST)-defined progression in melanoma. [11,12] Mechanisms to account for these atypical presentations include delayed antitumor response, as well as “pseudoprogression,” in which a transient immune infiltration causes a paradoxical enlargement of the tumor with subsequent shrinkage and clinical benefit that transcends response rate (eg, overall survival (OS) benefit independent of response rate). Two retrospective studies evaluated the benefit of anti–PD-1 antibody therapy past progression in patients with metastatic melanoma. [11,12] Impressive response rates of 19% and 28% were seen in evaluable patients treated beyond progression, with these cases representing 4% and 5% of all patients who had received PD-1 inhibition in these studies, respectively. Notably, delayed responses were rare after 6 months, with these events likely indicative of true progressive disease.
Does PD-1 inhibitor have immunomodulatory properties?
Targeting angiogenesis may also be an effective strategy to increase the efficacy of PD-1/PD-L1 inhibitors, since emerging data suggest that these agents possess immunomodulatory properties that may potentiate a durable immune response and/or overcome resistance. [64] A phase I study of combination bevacizumab and ipilimumab in patients with metastatic melanoma demonstrated a DCR of 67%, with provocative correlative data showcasing an intense immune infiltration in on-treatment tumor biopsies. [64] This prompted several additional trials across tumor types (ClinicalTrials.gov identifier: NCT02681549), including renal cell carcinoma: the phase II IMmotion150 trial demonstrated an improvement in PFS for PD-L1–positive patients (PD-L1 expression ≥ 1%) treated with combination atezolizumab/bevacizumab vs atezolizumab monotherapy. [65] The efficacy and safety of atezolizumab plus bevacizumab is currently under exploration in untreated melanoma patients with brain metastases (ClinicalTrials.gov identifier: NCT03175432).
How long should you take Keytruda?
In addition, labeling for Merck & Co. Inc.'s PD-1 inhibitor Keytruda (pembrolizumab) advises dosing for up to 24 months in patients without disease progression.
What is the catch-22 for immunotherapy?
The Catch-22 for the industry, however, is that shorter courses of treatment could mean reduced sales for immunotherapy drug sponsors. While there was general agreement that the idea of shorter durations of therapy requires further study, researchers and industry executives cited barriers to developing the data needed to change from ...
Why are randomized trials needed?
Randomized trials are needed to explore not just stopping early, but also possible predictors of success with an earlier stop, McDermott said, noting that optimal duration may depend, in part, on the type of cancer.
Is PD L1 a long term treatment?
Long-term or open-ended treatment with PD-1/PD-L1 inhibitors is a burden for patients and the healthcare system and does not fit the biological paradigm of cancer immunotherapies, experts say; however, challenges to studying shorter durations include fears of undertreatment and patient objections to stopping a therapy that appears to be working.
Is immunotherapy a burden?
Shorter durations of immunotherapy could mean less financial burden for payers and patients and reduced risk of long-term toxicities for patients, but also less revenue for drug sponsors. Unlimited immunotherapy treatment "is actually burdensome," said Israel Lowy, vice president of global clinical development and head of translational science ...
Overview
PD-1 inhibitors and PD-L1 inhibitors are a group of checkpoint inhibitor anticancer drugs that block the activity of PD-1 and PDL1 immune checkpoint proteins present on the surface of cells. Immune checkpoint inhibitors are emerging as a front-line treatment for several types of cancer.
PD-1 and PD-L1 inhibitors act to inhibit the association of the programmed de…
History
The concept of blocking PD-1 and PD-L1 for the treatment of cancer was first published in 2001. Pharmaceutical companies began attempting to develop drugs to block these molecules, and the first clinical trial was launched in 2006, evaluating nivolumab. As of 2017, more than 500 clinical trials involving PD-1 and PD-L1 inhibitors have been conducted in more than 20,000 patients. By the end of 2017, PD-1/PD-L1 inhibitors had been approved for the treatment of nine forms of can…
Cancer immunotherapy
In the cancer disease state, the interaction of PD-L1 on the tumor cells with PD-1 on a T-cell reduces T-cell function signals to prevent the immune system from attacking the tumor cells. Use of an inhibitor that blocks the interaction of PD-L1 with the PD-1 receptor can prevent the cancer from evading the immune system in this way. Several PD-1 and PD-L1 inhibitors are being trialled within the clinic for use in advanced melanoma, non-small cell lung cancer, renal cell carcinoma, bladd…
Therapeutics
Pembrolizumab (formerly MK-3475 or lambrolizumab, Keytruda) was developed by Merck and first approved by the Food and Drug Administration in 2014 for the treatment of melanoma. It was later approved for metastatic non-small cell lung cancer and head and neck squamous cell carcinoma. In 2017, it became the first immunotherapy drug approved for use based on the genetic mutations of the tumor rather than the site of the tumor. It was shown, that patients with higher non-synon…
Adverse effects
Immunotherapies as a group have off-target effects and toxicities common to them. Some of these include interstitial pneumonitis, colitis, hepatitis, thyroiditis, skin reactions, low levels of platelets and white blood cells, inflammation of the brain or spinal cord, neuromuscular adverse events including myositis, Guillain-Barré syndrome, myasthenia gravis; myocarditis and cardiac insufficiency, acute adrenal insufficiency, and nephritis. The most common kidney related chang…
See also
• Cancer immunotherapy - Immune checkpoints
• Intracellular checkpoints - CISH