3.1.2 Inhibitor characteristics
| Characteristics | Early inhibitor ( n = 63) | Late inhibitor ( n = 26) |
| Increased bleeding tendency (%) | 60 (95) | 24 (92) |
| Decreased baseline FVIII activity level ... | 39 (62) | 12 (46) |
| Unknown | 11 (18) | 5 (19) |
| Decrease of FVIII activity level <1% (%) | 21 (33) | 4 (15) |
Full Answer
Does intensive FVIII treatment increase the risk of inhibitor development?
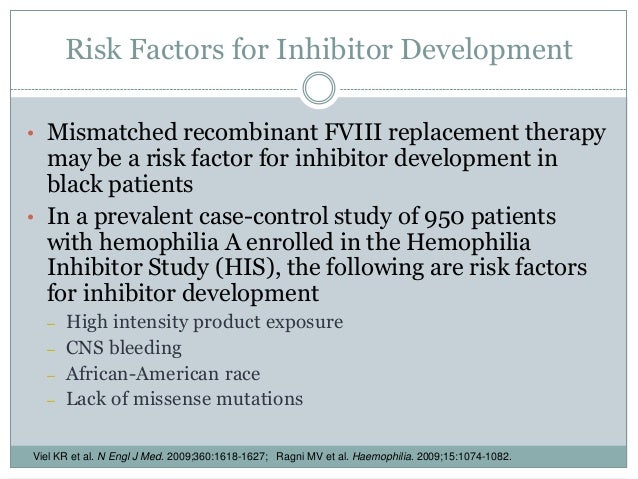
High-dose intensive FVIII treatment of bleeding or surgery was associated with an increased risk for the development of inhibitors. Correspondingly, prophylactic FVIII treatment was associated with a decreased risk for inhibitor development.
What are the different types of FVIII inhibitors?
FVIII inhibitors are classified based on the kinetics and extent of inhibition of FVIII. Type I inhibitors follow second-order kinetics (dose-dependent linear inhibition) and completely inactivate FVIII. Type II inhibitors have complex kinetics and incompletely inactivate FVIII.
What is the risk score for FVIII treatment?
The risk score is cumulative and includes two points for a positive family history of inhibitors, two points for a high-risk gene mutation and three points if the initial FVIII treatment is intensive.
What is a factor VIII inhibitor?
Inhibitors greatly reduce—or inhibit—the ability of the factor to stop bleeding, making it very hard to control or prevent bleeding episodes. Inhibitors can develop in up to 35% of people with severe hemophilia A who receive factor VIII (FVIII) replacement therapy.
What are the risks related to treatment of hemophilia?
ComplicationsDeep internal bleeding. Bleeding that occurs in deep muscle can cause the limbs to swell. ... Bleeding into the throat or neck. This can affect a person's ability to breathe.Damage to joints. ... Infection. ... Adverse reaction to clotting factor treatment.
Which factors are used for treatment of hemophilia A?
Emicizumab (Hemlibra) is a therapy used to treat hemophilia A, to prevent bleeding episodes in people both with and without inhibitors. It is known as a factor VIII(8) mimetic because it mimics, or imitates, the way factor VIII(8) works. It brings together factor IX(9) and factor X (10), which allows the blood to clot.
What are FVIII inhibitors?
FVIII inhibitors are classified based on the kinetics and extent of inhibition of FVIII. Type I inhibitors follow second-order kinetics (dose-dependent linear inhibition) and completely inactivate FVIII. Type II inhibitors have complex kinetics and incompletely inactivate FVIII.
What happens when factor VIII deficiency?
If the factor VIII gene is missing on a boy's X chromosome, he will have hemophilia A. For this reason, most people with hemophilia A are male. If a woman has a defective factor VIII gene, she is considered a carrier. This means the defective gene can be passed down to her children.
What intervention should be avoided in patients with hemophilia?
To avoid excessive bleeding and protect your joints: Exercise regularly. Activities such as swimming, bicycle riding and walking can build muscles while protecting joints. Contact sports — such as football, hockey or wrestling — are not safe for people with hemophilia.
How do you treat hemophilia with inhibitors?
About Inhibitors People with hemophilia, and many with VWD type 3, use treatment products called clotting factor concentrates (“factor”). These treatment products improve blood clotting, and they are used to stop or prevent a bleeding episode.
How are factor inhibitors treated?
Patients with low-titer inhibitors can be treated with plasma-derived or recombinant human FVIII concentrates, which should be administered at doses sufficient to overwhelm the inhibitor and thus achieve hemostatic levels of factor VIII.
What treatment options are available for a hemophiliac child who is bleeding and has a high factor VIII inhibitor titer?
Treatment options for bleeding BPAs provide hemostasis through pathways that circumvent the need for fVIII or fIX to generate thrombin. The 2 currently available BPAs are recombinant fVIIa (rfVIIa; Novoseven RT, Novo Nordisk) and activated prothrombin complex concentrate (aPCC; FEIBA VH, Baxalta).
What factors are in Feiba?
FEIBA contains mainly non-activated factors II, IX, and X and mainly activated factor VII. It contains approximately equal unitages of factor VIII inhibitor bypassing activity and prothrombin complex factors. In addition, the preparation contains 1-6 units of factor VIII coagulant antigen (F VIII C: Ag) per mL.
What technical errors could produce a decreased factor VIII?
If you have an abnormally low level of factor VIII, it could be caused by: an inherited factor VIII deficiency (hemophilia A) disseminated intravascular coagulation (DIC), a disease in which certain proteins responsible for blood clotting are abnormally active. the presence of a factor VIII inhibitor.
What is the role of factor VIII?
Factor VIII (FVIII) functions as a co-factor in the blood coagulation cascade for the proteolytic activation of factor X by factor IXa. Deficiency of FVIII causes hemophilia A, the most commonly inherited bleeding disorder.
Is von Willebrand factor the same as factor VIII?
Abstract. Factor VIIII (FVIII) and von Willebrand factor (VWF) are two distinct but related glycoproteins that circulate in plasma as a tightly bound complex (FVIII/VWF).
What are the main treatment challenges for hemophilia?
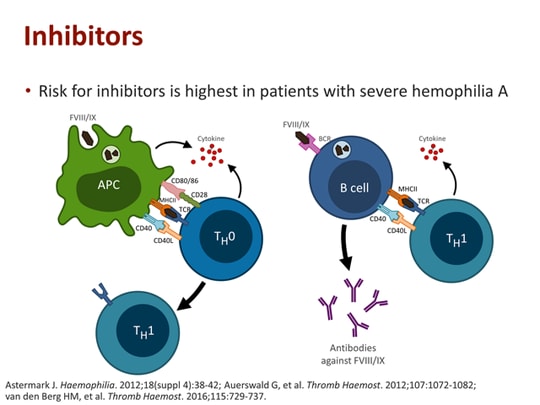
Inhibitors Are the Main Treatment Challenge Today 1. Inhibitors Are the Main Treatment Challenge Today. Inhibitors are a serious complication of hemophilia treatment in which the body's immune system develops antibodies (inhibitors) to the infused factor used to treat bleeding episodes. Inhibitors greatly reduce—or inhibit—the ability ...
What is the most serious complication of hemophilia A?
Inhibitors can develop in up to 35% of people with severe hemophilia A who receive factor VIII (FVIII) replacement therapy. Inhibitors attach to FVIII and diminish its ability to stop bleeding. Inhibitors are the most serious and challenging complication of hemophilia A management. 1,2.
What is inhibitor titer?
When choosing treatment options, a healthcare professional considers inhibitor titer, strength with which the body reacts to factor, site/severity of bleed, and other possible influences. People with low-titer inhibitors can sometimes continue to use factor concentrates but may need more.
Is hemophilia A at risk for inhibitors?
patients with hemophilia A are at risk of inhibitors, regardless of age and disease severity 4,5. PREVALENCE AND RISK OF INHIBITORS. The risk of inhibitor development in hemophilia A is significant. ~35% of people with severe hemophilia A may develop an inhibitor 2. ~25% of people with hemophilia A who develop an inhibitor will deal with ...
Can you test for inhibitors?
Yes. It is not always obvious that someone has developed an inhibitor, so regular testing and continuous care from a healthcare professional is recommended. It is common practice to test for inhibitors when people with hemophilia are not responding to their therapy.
What causes FVIII inhibitors?
In addition, there are other causes of inhibitor development against FVIII like stress, age, malignancy, infection, pregnancy, antibiotics, etc. Development of inhibitors in such cases happens in individuals who are not hemophilic and have normal plasma FVIII levels.
What is the most serious complication of factor VIII replacement therapy?
Development of inhibitors is perhaps the most serious complication of factor VIII (FVIII) replacement therapy, which can practically preclude efficient clinical management of patients with hemophilia A.
What is the model of anti-FVIII?
The causative FVIII mutation and HLA class II will be the main contributors to the risk of development of antibodies; from very low risk (green) unlikely to experience any antibodies with commercially available FVIII concentrates to very high risk (red). The final immune response and outcome will then be fine-tuned by T-regulatory cells and a variety of immune regulatory molecules, the activity of which will be defined genetically by therapy-related factors and immune system challenges.
Why is treatment of an inflammatory setting important?
It is possible that in an inflammatory setting in the presence of alert signals for the immune system, the amount of exposed antigen may be of relevance to risk.
Is anti-factor antibody multifactorial?
It is clear that the process is multifactorial and involves cells , cytokines, and other immune regulatory molecules, the level and action of which are both genetically and nongenetically defined. Despite improvements in understanding, we remain unable to fully predict the immune response to the deficient factor and inhibitor risk at the onset of replacement therapy. There are several ongoing efforts aiming to achieve more accurate methods for prediction and others to develop nonimmunogenic hemostatic options, but these remain opportunities for the future. Findings continue to emerge regarding risk factors and potential immune mechanisms of significance for the outcome, but until new results have been sufficiently confirmed through replication and the mechanisms of action in humans better defined, the chances of withholding a beneficial treatment or administering one associated with an adverse outcome are increased. Efficacy and safety should be the guiding principles for all treaters in the environment of cost constraints in which they act. This review will summarize current data-based findings and interpretations of how and why inhibitory antibodies develop in patients with hemophilia A and explore how the findings may or may not influence our daily practice.
What is the FVIII infusion?
The current standard of care of children with severe hemophilia A is primary prophylaxis: regular FVIII infusions aimed at prevention of joint damage that are started from the first joint bleeding onward or earlier. 1, 2
How many IU/kg infusions are there in FVIII?
To investigate the effect of the dose and frequency of FVIII infusions in prophylaxis, regular prophylaxis was categorized into 4 arbitrarily defined categories of prophylaxis: (1) once a week, less than 30 IU/kg/infusion; (2) once a week, more than 30 IU/kg/infusion; (3) more than once a week, less than 30 IU/kg/infusion; and (4) more than once a week, more than 30 IU/kg/infusion. On-demand treatment was the reference.
How many patients started prophylaxis?
A total of 412 patients (71.5%) started regular prophylaxis within the first 75 exposure days. Patients started prophylaxis at a median age of 16.7 months (IQR, 12.4-24.4 months) and after a median number of 15 exposure days (IQR, 7-25 days). Twenty-five patients started prophylactic treatment from the first exposure onward. The crude and adjusted relative risks for inhibitor development according to the treatment regimen (on demand or prophylaxis) are presented in Table 4.
How long is the cumulative inhibitor incidence curve?
For this reason, we also estimated the values of the HR allowing it to vary during 75 exposure days. The period of 1 to 75 exposure days was categorized into arbitrarily defined periods (1-10, 11-20, 21-30, 31-40, and 40-75 days).
What are the different types of hemophilia?
Apparently, there are 3 types of patients with severe hemophilia A: (1) patients in whom inhibitors will never develop; (2) patients in whom inhibitor development depends on the treatment regimen; and (3) patients in whom inhibitors will develop in all situations.
Why is prophylaxis not always clear cut?
Ascertaining the moment when prophylaxis was truly started is not always clear-cut, because of venous access problems or lack of cooperation of the child. Therefore, we defined prophylaxis in 2 ways, analogous with the analysis of randomized controlled trials: the “per-protocol analysis” and “intention-to-treat analysis.”
Does prophylaxis have the same inhibitors as on demand?
A new and rather surprising finding was that during the first 20 exposure days, patients receiving prophylaxis had exactly the same inhibitor risks as the patients treated on demand. In this study, the frequency and dose of prophylaxis were not associated with the risk for inhibitor development.
