Nutrition
Kanamycin, Capreomycin and Amikacin are injectable second-line. XDR TB occurs when a Mycobacterium tuberculosis strain is resistant to isoniazid and rifampin, two of the most powerful first-line drugs, as well as key drugs of the second line regimen—any fluoroquinolone and at least one of the three injectable drugs shown above.
What is the second line treatment for XDR tuberculosis (TB)?
The standard of care for initiating treatment of TB disease is four-drug therapy. Treatment with a single drug can lead to the. development of a bacterial population resistant to that drug.
What are the treatment options for tuberculosis (TB) disease?
When two or more drugs to which in vitro susceptibility has been demonstrated are given together, each helps prevent the emergence of tubercle bacilli resistant to the others. The standard of care for initiating treatment of TB disease is four-drug therapy. Treatment with a single drug can lead to the
Why are two or more drugs given together in tuberculosis (TB)?
In 2019 WHO published new consolidated guidance on the second line drugs to be used for the treatment of drug resistant TB. 2"WHO consolidated guidelines on drug-resistant tuberculosis treatment", 2019, Geneva, https://www. who.
What is the who's new guidance on drug-resistant tuberculosis (TB)?

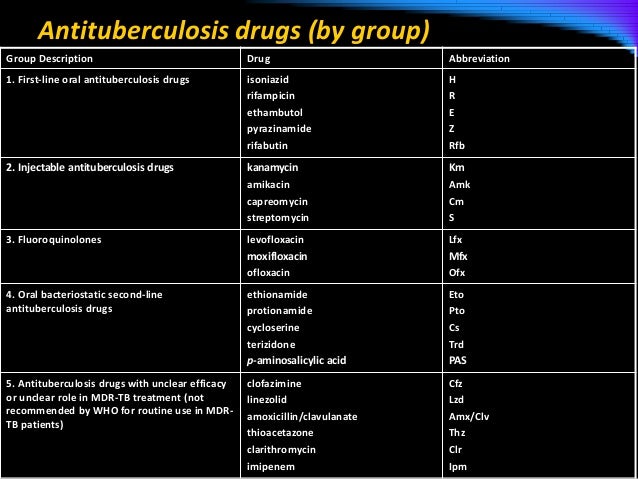
What are the second-line drugs for TB?
Kanamycin, Capreomycin and Amikacin are injectable second-line. Bedaquiline and Delamanid are new drugs. Ethambutol, Pyrazinamide, Thioamides, Cycloserine, Para-aminosalicylic acid, Streptomycin, and Clofazimine are possibly effective.
What is the second phase of TB treatment?
The preferred continuation-phase regimen is four months of rifampicin and isoniazid (4RH) administered daily or three times weekly. The main advantage of this regimen is the low rate of treatment failure and relapse for patients with fully susceptible TB or TB with initial resistance to isoniazid.
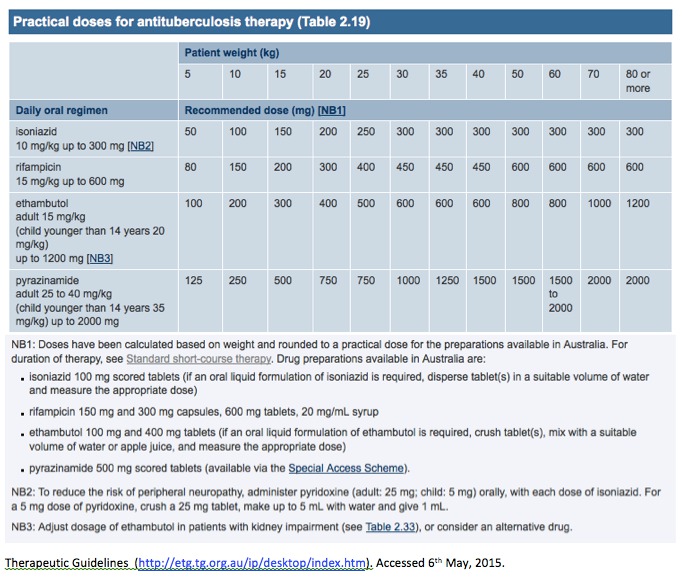
What are the 4 drug regimen given to patients with tuberculosis?
For initial empiric treatment of TB, start patients on a 4-drug regimen: isoniazid, rifampin, pyrazinamide, and either ethambutol or streptomycin. Once the TB isolate is known to be fully susceptible, ethambutol (or streptomycin, if it is used as a fourth drug) can be discontinued.
What are the phases of tuberculosis patients treatment?
Regimens for treating TB disease have an intensive phase of 2 months, followed by a continuation phase of either 4 or 7 months. The continuation phase should be extended to 28 weeks for patients who have cavitation on the intensive chest film and positive sputum cultures after 2 months of treatment.
What is a second line medication?
Any therapeutic agent that is not the drug of choice, or the 1st normally used to treat a particular condition; in rheumatoid arthritis, 2nd-line agents are used when standard 'first-line' therapy–ie, anti-inflammatory agents and corticosteroids fail.
What are first and second line drugs of tuberculosis?
Injectable antituberculosis drugs- Kanamycin (KAN), amikacin (AMK) and capreomycin (CAP). Less-effective second-line antituberculosis drugs- Ethionamide (ETH)/Prothionamide (PTH), Cycloserine (CS)/Terizidone, P-aminosalicylic acid (PAS).
What is the standard TB treatment regimen?
The preferred regimen for treating adults with TB remains a regimen consisting of an intensive phase of 2 months of isoniazid (INH), rifampin (RIF), pyrazinamide (PZA), and ethambutol (EMB) followed by a continuation phase of 4 months of INH and RIF.
What are 3 drugs for TB?
Pulmonary TB 2 antibiotics (isoniazid and rifampicin) for 6 months. 2 additional antibiotics (pyrazinamide and ethambutol) for the first 2 months of the 6-month treatment period.
WHO TB treatment guideline?
Current policy recommendations on treatment and care for DR-TB. In patients with confirmed rifampicin-susceptible and isoniazid-resistant tuberculosis, treatment with rifampicin, ethambutol, pyrazinamide and levofloxacin is recommended for a duration of 6 months.
What is the first line drug for TB?
First-line agents for treatment of active TB consist of isoniazid, a rifamycin (rifampin or [less frequently] either rifapentine or rifabutin), pyrazinamide, and ethambutol; in addition, moxifloxacin is a first-line agent when administered in combination with isoniazid, rifapentine, and pyrazinamide [6].
What drug class is rifampin?
Rifampin is in a class of medications called antimycobacterials. It works by killing the bacteria that cause infection. Antibiotics such as rifampin will not work for colds, flu, or other viral infections.
What is the second line of treatment for drug resistant TB?
Second line drugs for treatment of drug resistant TB (as of March 2019) WHO now recommends that all oral regimens should become the preferred option for most patients. It is a major step forward in the treatment of patients with drug resistant TB that most patients will no longer be required to have injectable drugs.
What are the second line drugs?
Second line drugs are the TB drugs that are used for the treatment of drug resistant TB. The second line drugs include levofloxacin, moxifloxacin, bedaquiline, delamanid and linezolid. There is also pretomanid which is a new second line drug recommended in 2019 for the treatment of drug resistant TB.
What is the second line of Amikacin?
Amikacin, a second line injectable drug. In 2019 WHO published new consolidated guidance on the second line drugs to be used for the treatment of drug resistant TB. 2"WHO consolidated guidelines on drug-resistant tuberculosis treatment", 2019, Geneva, https://www.who.int/tb/publications/2019/consolidated-guidelines-drug-resistant-TB-treatment/en/ ...
Who recommends all oral regimens?
WHO now recommends that all oral regimens should become the preferred option for most patients. It is a major step forward in the treatment of patients with drug resistant TB that most patients will no longer be required to have injectable drugs.
What is the new drug for TB?
Bedaquiline and Delamanid are new drugs. Ethambutol, Pyrazinamide, Thioamides, Cycloserine, Para-aminosalicylic acid, Streptomycin, and Clofazimine are possibly effective. Kanamycin, Capreomycin and Amikacin are injectable second-line. XDR TB occurs when a Mycobacterium tuberculosis strain is resistant to isoniazid and rifampin, ...
How to cure MDR TB?
To cure MDR TB, healthcare providers must turn to a combination of second-line drugs, several of which are shown here. Second-line drugs may have more side effects, the treatment may last much longer, and the cost may be up to 100 times more than first-line therapy. MDR TB strains can also grow resistant to second-line drugs, ...
What drugs target DNA?
Rifamycins, Oxazolidinones and Macrolides act on DNA. Tuberculosis drugs target various aspects of Mycobacterium tuberculosis biology, including inhibition of cell wall synthesis, protein synthesis, or nucleic acid synthesis. For some drugs, the mechanisms of action have not been fully identified.
Who took the photo of Mycobacterium tuberculosis?
The photo of Mycobacterium tuberculosis is from the Centers for Disease Control and Prevention, CDC/Dr. Ray Butler, Janice Carr. This illustration is in the public domain. Please credit the National Institute of Allergy and Infectious Diseases (NIAID).
Is XDR TB resistant to isoniazid?
NIAID. XDR TB occurs when a Mycobacterium tuberculosis strain is resistant to isoniazid and rifampin, two of the most powerful first-line drugs, as well as key drugs of the second line regimen—any fluoroquinolone and at least one of the three injectable drugs shown above. XDR TB strains may also be resistant to additional drugs, ...
Why is it important to take TB medication?
But it is crucial to complete the full course of therapy, because skipping doses or stopping treatment too soon may result in the growth of bacteria that are resistant to one or more medications. This leads to a TB infection that is more difficult and expensive to treat. It also increases the risk of relapse after treatmet is completed.
How long does isoniazid last in South Africa?
In South Africa, IPT is available in public clinics for people living with HIV. IPT reduces a person’s risk of developing active TB. The standard regimen is 300 mg daily of isoniazid for 6-9 months in adults and adolescents and 5 mg/kg for children. The World Health Organisation now recommends an even longer course of 36 months. However, it is important that IPT only be given to patients who are tuberculin skin test-positive. Long-term IPT may actually be harmful when given to people who are tuberculin skin test-negative.
Why do people with TB test positive for HIV?
Many people with tuberculosis also test positive for HIV. This is because a weakened immune system enables tuberculosis infection to develop more easily . In addition, TB speeds up the course of an HIV infection. South Africa has one of the highest rates of TB/HIV co-infection, with 73% of those infected with tuberculosis testing positive for HIV.[i] Therefore it is recommended that all patients with TB be given counseling and testing for HIV infection. TB/HIV co-infected patients should receive antiretroviral treatment regardless of their CD4 count. People diagnosed with TB and HIV should start TB treatment and then begin antiretroviral treatment within two to four weeks.
What are the best drugs for TB?
The drugs that a patient should take depends on whether the patient has ever had TB treatment before. If the patient has never had treatment before then it can be assumed that the bacteria in the patient's body will respond, and be sensitive to all the TB drugs. So the patient can then be given the following drugs: 1 Isoniazid 2 Rifampicin 3 Pyyrazinamide 4 & Ethambutol.
How many drugs are there for TB?
There are more than twenty drugs available for TB treatment. Which ones have to be taken depends on the circumstances of the patient. If you are having TB treatment (sometimes known as antitubercular treatment or ATT), then this should always be supervised by an experienced doctor or other health person.
Why does TB treatment fail?
It is often suggested that TB treatment fails because a patient doesn’t take their TB drugs correctly. However there can be a number of different reasons for TB treatment failure. It is certainly true that if a patient doesn’t take their TB drugs properly that this can lead to the development of drug resistant TB.
What is the second exception to isoniazid?
The second exception is if the patient has been known to be in contact with a patient who is known to have drug resistant TB.
What is the responsibility of a doctor for TB?
A patient must take their drugs properly. But it is also the responsibility of the doctor to make sure that the patient has the correct drugs. The doctor must also explain to the patient how to take the drugs correctly. In many countries there are "alternative" medicines available.
What happens if you take only one or two TB drugs?
If only one or two TB drugs are taken then only some of the bacteria may be killed. They may then become resistant to the TB drugs which then don't work. If the person becomes sick again then different TB drugs called second line drugs may be needed.
How often should I take isoniazid?
Isoniazid. plus rifampicin. for the continuation treatment phase. It is recommended that patients take the TB drugs every day for six months. Taking the drugs three times a week used to be considered satisfactory but is no longer recommended by the WHO. It is essential that all the recommended TB drugs are taken.
What are the drugs that treat TB?
Food and Drug Administration (FDA) for the treatment of TB disease (Table 6.2). In addition, the fluoroquinolones (levofloxacin, moxifloxacin, and gatifloxacin), although not approved by the FDA for TB disease, are commonly used to treat TB disease caused by drug-resistant organisms or for patients who are intolerant of some first-line drugs. Rifabutin, approved for use in preventing Mycobacterium avium complex disease in patients with HIV infection but not approved for TB disease, is useful for treating TB disease in patients concurrently taking drugs that interact with rifampin (e.g., certain antiretroviral drugs). Amikacin and kanamycin, nearly identical aminoglycoside drugs used in treating patients with TB disease caused by drug-resistant organisms, are not approved by the FDA for treatment of TB.
How long does it take to treat TB?
As a general rule, the principles used for the treatment of pulmonary TB disease also apply to extrapulmonary forms of the disease. A 6-month treatment regimen is recommended for patients with extrapulmonary TB disease, unless the organisms are known or strongly suspected to be resistant to the first-line drugs. If PZA cannot be used in the initial phase, the continuation phase must be increased to 7 months. The exception to these recommendations is central nervous system TB, for which the optimal length of therapy has not been established but some experts recommend 9 to 12 months. Most experts do recommend corticosteroids to be used as additional therapy for patients with TB meningitis and pericarditis. Consultation with a TB expert is recommended.
What are the four drugs that are included in the initial treatment regimen?
Four drugs— INH, RIF, PZA, and EMB — should be included in the initial treatment regimen until the results of drug-susceptibility tests are available. Each of the drugs in the initial regimen plays an important role. INH and RIF allow for short-course regimens with high cure rates. PZA has potent sterilizing activity, which allows further shortening of the regimen from 9 to 6 months. EMB helps to prevent the emergence of RIF resistance when primary INH resistance is present. If drug-susceptibility test results are known and the organisms are fully susceptible, EMB need not be included. For children whose clarity or sharpness of vision cannot be monitored, EMB is usually not recommended except when the risk of drug resistance is high or for children who have “adult-type” (upper lobe infiltration, cavity formation) TB disease.
How long is the TB continuation phase?
The continuation phase of treatment is given for either 4 or 7 months. The 4-month continuation phase should be used in patients with uncomplicated, noncavitary, drug-susceptible TB, if there is documented sputum conversion within the first 2 months. The 7-month continuation phase is recommended only for
What is the recommended treatment regimen based on?
The recommended treatment regimens are based, in large part, on evidence from clinical trials and are rated on the basis of a system developed by the U.S. Public Health Service (USPHS) and the Infectious Diseases Society of America (IDSA) (Table 6.3).
How to educate patients about TB?
Educating patients about TB disease helps ensure their successful completion of therapy. Health-care providers must take the time to explain clearly to patients what medication should be taken, how much, how often, and when. Patients should be clearly informed about possible adverse reactions to the medications they are taking and when to seek necessary medical attention. Providing patients with the knowledge they need regarding the consequences of not taking their medicine correctly is very important. In addition, patients should be educated about infection control measures and potential need for isolation (Table 6.1). HIV testing and counseling is recommended for all patients with TB disease in all health-care settings. The patient must first be notified that testing will be performed. The patient has the right to decline HIV testing and counseling (opt-out screening).
How long does it take to develop a TB control plan?
For each patient with newly diagnosed TB disease, a specific treatment and monitoring plan should be developed in collaboration with the local TB control program within 1 week of the presumptive diagnosis. This plan should include: