At their best, DSM diagnoses help social workers and other mental health professionals understand clients, guiding their interventions from an evidence-based perspective. Diagnosis helps professionals with goal setting, treatment planning, and determining a client’s prognosis. Having a common nomenclature for diagnoses also facilitates research.
Full Answer
How is the DSM used in clinical psychology?
Clinicians rely on self-reported and observable presenting symptoms from their patients and assess them using the DSM to diagnosis their patient. The DSM also provides a basis for research and treatment to further the collection of empirical evidence in psychology.
How can counsellors use the DSM-5?
Counselors have the opportunity to use the DSM-5, provide feedback directly to the APA, and help shape and influence future editions of this diagnostic tool. This is an important way counselors can advocate for their clients as well as their profession, and shape how the DSM is used to help treat those suffering from mental and emotional distress.
What is the purpose of the DSM 3?
This diagnosis assists the clinician in how they will proceed with treatment for the patient. The third section of the manual goes into a further description of each disorder and its subsets. The DSM is only for use by trained professionals as a diagnostic tool in treating psychological disorders.
Should social workers use the DSM?
Despite the widespread use of the DSM, social workers should be cognizant of the ethical issues that may arise in the context of using this diagnostic tool.

Does the DSM include treatment plans?
DSM-5-TR, like DSM-5, is a manual for assessment and diagnosis of mental disorders and does not include information or guidelines for treatment of any disorder.
How is the DSM used during the diagnostic process?
The DSM provides an important standardisation of diagnostic categories for psychiatric research and treatment. Prior to the this system, there were substantial variations in the way certain diagnoses were applied. This made clinical diagnosis inconsistent and substantial advances in psychiatric research impossible.
How do you make a diagnosis using the DSM-5?
Six Steps to Better DSM-5 Differential DiagnosisStep 1: Rule Out Malingering and Factitious Disorder. ... Step 2: Rule Out Substance Etiology. ... Step 3: Rule Out Disorder Due to a General Medical Condition. ... Step 4: Determining the Specific Primary Disorder.More items...•
How would a therapist utilize the DSM-5?
Therapists use the DSM-5 to: Identify and diagnose mental health conditions. Differentiate between similar diagnoses and ensure that the most appropriate treatment is provided. Identify the proper diagnosis for submitting claims to health insurance companies so clients can receive coverage for their sessions.
What are the 5 DSM categories?
Example categories in the DSM-5 include anxiety disorders, bipolar and related disorders, depressive disorders, feeding and eating disorders, obsessive-compulsive and related disorders, and personality disorders.
What is the goal of DSM-5?
A key goal of DSM-5 was to create a more dimensional characterization of psychiatric disorders, juxtaposed on the traditional categorical diagnostic classifications. There are several diagnostic groups for which there were few, if any, major changes in diagnostic criteria.
Why is DSM-5 important to the study and treatment of psychological disorders?
Research Guidance. In addition, the DSM helps guide research in the mental health field. The diagnostic checklists help ensure that different groups of researchers are studying the same disorder—although this may be more theoretical than practical, as so many disorders have such widely varying symptoms.
Why do counselors use the DSM-5?
Even professionals who are not traditionally responsible for diagnosis as a part of their counseling services, such as school or career counselors, should understand the DSM so they can recognize diagnostic problems or complaints and participate in discussions and treatment regarding these issues.
What is DSM in counseling?
DSM-5 is the standard diagnostic manual published with criteria and definitions of mental disorders published by the American Psychiatric Association (APA). It is the diagnostic manual most frequently used by counselors in the US,.
What changes should counselors consider to the DSM-5?
Counselors should consider the aforementioned changes to the DSM-5 in the context of their counselor identity. Maintaining professional identity and promoting a wellness- and strength-based perspective continues to be an important concern for the counseling profession and the training of counselors. Tomlinson-Clarke and Georges (2014) provide an overview of maintaining professional identity in the process of assessment and diagnosis within a system representing the medical model. A particular strength is the inclusion of how multicultural competency is crucial in using the DSM-5 effectively, which is an essential basic foundation to sound practice. Implications for counselor preparation also are a focus. Finally, Frances (2014) provides a critical commentary of how the DSM has been used by pharmaceutical companies to leverage significant profits at the cost to consumers of mental health services and our economy. As the former chair of the DSM-IV task force, Frances reminds counselors and other mental health professionals of their essential place within treatment and cautions counselors to use the DSM in a balanced manner. His comments are consistent with advocacy inherent in our profession for treatments that promote client resilience, and address psychosocial and environmental factors that impact client functioning.
What is the importance of the DSM-5?
An important emphasis within the DSM-5 is substance-use and substance-induced disorders, which are included in many relevant diagnostic criteria (APA, 2013). Counselors are well-advised to make this determination in the initial assessment and continue to assess throughout the course of treatment.
What is the CFI in the DSM?
Two decades of experience using the Outline for Cultural Formulation (OCR), which was introduced in the DSM-IV (APA, 1994), evolved into the Cultural Formulation Interview (CFI) now contained in the DSM-5, comprised of 16 semi-structured questions designed to collect data in a more consistent and efficient manner. Like other dimensional, cross-cutting and severity measures developed specifically for the DSM-5, the CFI was field tested at 12 sites representing several countries to determine feasibility and usefulness (Lewis-Fernández et al., 2014). For the first time, culture in its varied manifestations has been intentionally incorporated into the DSM nosology through a specific assessment instrument. “The CFI follows a person-centered approach to cultural assessment…designed to avoid stereotyping, in that each individual’s cultural knowledge affects how he or she interprets illness experience and guides how he or she seeks help” (APA, 2013, p. 751). Counselors are encouraged to utilize the CFI as a way to understand their clients more meaningfully and to aid in clinical utility.
What is the DSM-5?
The fifth edition of the Diagnostic and Statistical Manual for Mental Disorders ( DSM-5) is an update of a major diagnostic tool (APA, 2013). The manual was originally designed to help mental health professionals within a wide variety of disciplines assess and conceptualize cases in which people were suffering from mental distress. This conceptualization is important in that it facilitates an understanding in a common language toward the development of treatment planning to address complex and entrenched symptomology. The DSM has undergone numerous iterations and represents the current knowledge of mental health professionals about mental illness (APA, 2013). One of the primary aims of the DSM-5 workgroups was to align the manual with the current version of the International Classification of Diseases ( ICD-9 ). In addition, political, social, legal and cultural dynamics influenced the development of the DSM-5 —and not without controversy (Greenberg, 2013; Locke, 2011; Linde, 2010; Pomeroy & Anderson, 2013). As with any tool, concerns have emerged about the potential of misuse. It is the professional responsibility of skilled and ethical mental health counselors and other professionals to prevent misapplication of the manual (American Counseling Association [ACA], 2014, E.1.b, E.5.a–d). Walsh (2007) succinctly noted that “the primary goal of the DSM is to enhance the care of individuals with psychiatric disorders” (p. S3).
What is considered a mental disorder?
The definition of mental disorder has not changed significantly from previous versions of the DSM: a mental disorder is “a syndrome characterized by clinically significant disturbance in…cognition, emotion regulation, or behavior that reflects a dysfunction in the psychological, biological, or developmental processes… [and] usually associated with significant distress or disability in social, occupational, or other important activities” (APA, 2013, p. 20). Identifying mental disorders, or the process of diagnosis, involves more than clear-cut observations and often includes the consideration of complex factors involving comorbidity, symptom clusters “that may be part of a more complex and unified syndrome that has been artificially split in the diagnostic system” (Nussbaum, 2013, p. 202), overlap between diagnostic criteria, genetic predisposition, and the mutual influence of two or more conditions. Counselors must be careful to consider the presence of these factors, consult when necessary, and take into account differential diagnosis to determine the most appropriate diagnosis given the verbal and observable data available.
Why is it important to differentiate disorder from non-disorder?
to help clinicians differentiate disorder from non-disorder for the purpose of determining who might benefit from disorder-based treatments. (First, 2010, p. 466)
Who uses the DSM IV?
The introduction of the DSM-IV-TR states that the DSM has been used by numerous mental health practitioners (APA, 2000), with no mention of their investment as legitimate stakeholders in the process of DSM development. Well before the final revision of the DSM-5, various mental health professionals, organizations and other relevant collaborators helped formulate the manual in unprecedented capacities. In the introduction to the DSM-5 (APA, 2013) the authors intentionally state that numerous stakeholders were involved in DSM-5 development including counselors and “patients, families, lawyers, consumer organizations, and advocacy groups” (p. 6). Of particular note was the inclusion of national organizations such as the ACA in the form of a DSM-5 task force, which submitted position statements and recommendations to the APA. Various mental health professionals participated directly in the formulation of the DSM-5, primarily in field trials which “supplied valuable information about how proposed revisions performed in everyday clinical settings” (p. 8). Much of the data supports the use of more than 60 cross-cutting and severity symptom measures (see http://www.psychiatry.org/practice/dsm/dsm5/online-assessment-measures ).
Why do clinicians use the DSM?
Clinicians rely on self-reported and observable presenting symptoms from their patients and assess them using the DSM to diagnosis their patient. The DSM also provides a basis for research and treatment to further the collection of empirical evidence in psychology. Using this tool, clinicians and researchers can develop new ways to combat symptoms and treat disorders.
What is the DSM?
Source: commons.wikimedia.org. The Diagnostic and Statistical Manual of Mental Disorders (DSM) is a tool used by mental health professionals to diagnose various mental illnesses. Though controversial for many reasons, this tool has been helpful since its first publishing in 1952 by the American Psychiatric Association (APA).
Why was the DSM created?
Initially, published in 1952, the DSM arose from an increased need for a standardized way of categorizing disorders that were presenting symptoms in the population. With the field of psychology continually progressing, it needed constant revisions over time to accommodate newly discovered disorders, changes made in classification, and other influencing factors. Before the official publishing of the DSM, psychological professionals used a single category to collect statistical information on the population.
How many disorders are in the DSM IV?
297 disorders were included in the DSM-IV.
What are the sections of the DSM?
The APA breaks the DSM up into three sections: the diagnostic classification, the diagnostic criteria sets, and the descriptions. The first section is a complete list of psychiatric disorders. The DSM codes each one for both diagnostic and billing purposes for health professionals. It dedicates the second section to how to identify psychological ...
What to do if you have a mental disorder?
If you believe you are exhibiting symptoms of a mental disorder, it is imperative to seek treatment immediately. Symptoms can be tricky and might mask themselves as other issues, so it is important to see a doctor as soon as possible to rule out any other potential health issues. Once you have a clear idea of what is going on, your doctor can recommend a specialist who can help guide you in the right direction.
Why do people get incorrect treatment?
In the past, due to social biases, many people received incorrect treatment. For example, people would receive a diagnosis of "hysteria," but it could have been a side effect of cultural expectations, environmental influences, and other potential disorders.
What are the changes to the DSM-5?
First, the DSM-IV-TR language has shifted from “threat to the physical integrity of self or others ” (APA, 2000, p. 467) to “sexual violence” (APA, 2013, p. 271). Second, the DSM-5 removed the DSM-IV-TR criterion A2 “subjective fear-based distress” because not all traumatized individuals experience fear, terror or horror when exposed to a trauma stressor. Some traumatized individuals may become anhedonic, dysphoric, aggressive or phobic; experience arousal and reactive-externalizing behaviors; or experience dissociation. Third, a new trauma exposure source is added to the traditional DSM-IV-TR trauma sources (i.e., directly experiencing, witnessing, and learning that a traumatic event occurred to a close family member or friend): “experiencing repeated or extreme exposure to aversive details of the traumatic event (s)” (APA, 2013, p. 271). An important note regarding this new exposure source in the DSM-5 indicates that “criterion A4 does not apply to exposure through electronic media, television, movies, or pictures, unless exposure is work related” (APA, 2013, p. 271). Examples of work-related electronic media exposure may include an individual who edits graphic news video or pictures, an individual who performs frequent digital-based forensic science investigations of graphic crime scenes, or an individual who views military-oriented electronic images displaying graphic human remains captured from unmanned aerial vehicles. Fourth, the DSM-5 requires that an individual manifest at least one symptom from each of the following pathological clusters:
What is clinical scenario in DSM-5?
Following the summary of changes, a clinical scenario is presented so that counselors can capture the vision of using the DSM-5 in their counseling practice. Clinical formulation (sample diagnosis) using the DSM-5 is also presented for each disorder classification.
What is the DSM-5 for autism?
The DSM-5 further recognizes autism due to Rett syndrome, Fragile X syndrome, Down syndrome, epilepsy, valproate, fetal alcohol syndrome or very low birth weight through use of the specifier associated with a known medical or genetic condition or environmental factor. Counselors also may use the specifiers with or without accompanying intellectual impairment and with or without accompanying language impairment. Examples of descriptive specifier usage include with accompanying language impairment—no intelligible speech or with accompanying language impairment—phrase speech. If catatonia is present, counselors record that separately as catatonia associated with autism spectrum disorder. Severity, or intensity of symptoms, for autism spectrum disorder are now communicated on three levels: Level 1 mild requiring support, level 2 moderate requiring substantial support, and level 3 severe requiring very substantial support (APA, 2013).
What is the DSM IV TR chapter?
The DSM-IV-TR chapter “Dementia, Delirium, Amnestic, and Other Cognitive Disorders ” is renamed to “Neurocognitive Disorders” (NCDs) in the DSM-5. Cognitive impairments occur in most mental disorders, including schizophrenia, bipolar disorder, depression, attention-deficit/hyperactivity disorder and autism (APA, 2013). However, the DSM-5 NCDs work group focused on those disorders for which the cognitive deficit is the primary one and is attributable to known physical or metabolic brain disease—hence the designation neurocognitive (Campbell, 2013).
What is probable in DSM-5?
The DSM-5 offers two new NCD designations: probable and possible. Probable is added to the diagnostic title if there is evidence of a causative disease genetic mutation from either genetic testing, evidence of family history, evidence from laboratory blood testing, or evidence from neuroimaging. Possible is used if there is no evidence resulting from the previously mentioned probable objective factors (APA, 2013). Counselors also may use the retained DSM-IV-TR descriptive specifier, without or with behavioral disturbance to indicate the presence of psychotic symptoms, mood disturbance, agitation, apathy or other behavioral symptoms.
What is insomnia based on?
The insomnia-based sleep-wake disorders focus on problems with initiating or maintaining quality sleep. Some of these disorders preclude assessment by a counselor, as they require examination by a sleep medicine expert. The DSM-IV-TR primary insomnia and insomnia related to another mental disorder are merged in the DSM-5 to become insomnia disorder. The DSM-IV-TR primary hypersomnia and hypersomnia related to another mental disorder are merged to become the DSM-5 hypersomnolence disorder. Narcolepsy is retained in the DSM-5 with substantial symptom description changes, five new specifiers and requirements for sleep medicine examination to confirm a diagnosis. Narcolepsy now requires either the presence of cataplexy (sudden loss of muscle tone), hypocretin deficiency as measured using cerebrospinal fluid, or REM sleep latency deficiency as measured using polysomnography (APA, 2013). Breathing-related sleep disorders in the DSM-5 include obstructive sleep apnea hypopnea, central sleep apnea (new for the manual) and sleep-related hypoventilation (new for the manual). Circadian rhythm sleep-wake disorders in the DSM-5 no longer recognize jet lag, resulting in five types (i.e., delayed sleep phase, advanced sleep phase, irregular sleep-wake, non-24-hour sleep-wake and shift work) for counselors to select when diagnosing this syndrome. Parasomnias, defined as abnormal behavior or physiological events during sleep, also are reconceptualized in the DSM-5. The DSM-IV-TR sleepwalking disorder and sleep terror disorder are merged to become the DSM-5 non–rapid eye movement sleep arousal disorder, with sleepwalking type, sleep-related eating, sleep-related sexual behavior, and sleep terror type specifiers (APA, 2013). Nightmare disorder is retained with no substantial changes from the DSM-IV-TR. The DSM-IV-TR parasomnia not otherwise specified is renamed in the DSM-5 to rapid eye movement sleep behavior disorder for disruptive dream enacting behaviors, and DSM-IV-TR dyssomnia not otherwise specified is renamed in the DSM-5 to restless legs syndrome.
What is the CRDPSS scale?
2013). Counselors can obtain the CRDPSS in the DSM-5 pages 742–744 (APA, 2013) or www.psychiatry.org/dsm5. The CRDPSS is an eight-item measure used to assess the severity of mental health symptoms that are important across psychotic disorders. These symptoms include delusions, hallucinations, disorganized speech, abnormal psychomotor behavior, negative symptoms (i.e., restricted emotional expression or avolition), impaired cognition, depression and mania. Psychosis symptoms are rated on a five-point scale: not present, equivocal (severity or duration not sufficient to be considered psychosis), mild (little pressure to act, not very bothered by symptoms), moderate (some pressure to respond or somewhat bothered by symptoms) and severe (severe pressure to respond to voices or very bothered by voices).
Why use DSM?
At their best, DSM diagnoses help social workers and other mental health professionals understand clients, guiding their interventions from an evidence-based perspective. Diagnosis helps professionals with goal setting, treatment planning, and determining a client’s prognosis. Having a common nomenclature for diagnoses also facilitates research. Despite the widespread use of the DSM, social workers should be cognizant of the ethical issues that may arise in the context of using this diagnostic tool.
What is the DSM 5?
The Diagnostic and Statistical Manual of the American Psychiatric Association, Fifth Edition (DSM 5) is known as the primary method of classification used by American mental health clinicians to diagnose patients with mental illnesses and conditions ( http://www.dsm5.org ). Diagnosis refers to a process of gathering information to understand a client’s condition, linking that information with knowledge about various cognitive, emotional, and behavioral conditions. The DSM is commonly referenced by social workers, particularly by clinical social workers practicing in the field of mental health.
What is the diagnosis of mental illness?
Diagnosing mental illnesses, however, is essentially an exercise in judging clients and focusing on their pathologies or weaknesses. When a social worker diagnoses a client with schizophrenia, for instance, the worker is highlighting problematic factors such as hallucinations, delusions, and paranoia.
What is the role of a social worker in the DSM?
When using the DSM to diagnose, social workers assume the role of expert, taking responsibility for determining which mental conditions clients have , rather than involving clients as full partners in the decision-making process. For instance, a social worker informs a client that he has depression rather than inviting the client to jointly explore whether he has concerns regarding depression.
What is holistic assessment?
A holistic assessment highlights client strengths and considers clients in the context of their social environments, including their family, friends, co-workers, neighbors, and other social support systems. A holistic assessment includes psychological functioning and problems, but also includes social functioning, spirituality, physical health, ...
Why is the DSM 5 omitted?
The DSM-5 has omitted a number of diagnostic categories used in its previous editions, because they lacked validity and research support.
What is empowerment in the healthcare industry?
“Empowerment” refers to providing clients with time, space, support, and other conditions that allow them to have greater control over their lives. Empowerment demonstrates respect for the dignity and worth of clients by treating clients as autonomous individuals with the right to make choices and decisions throughout the helping process (NASW Code of Ethics, Standard 1.02).
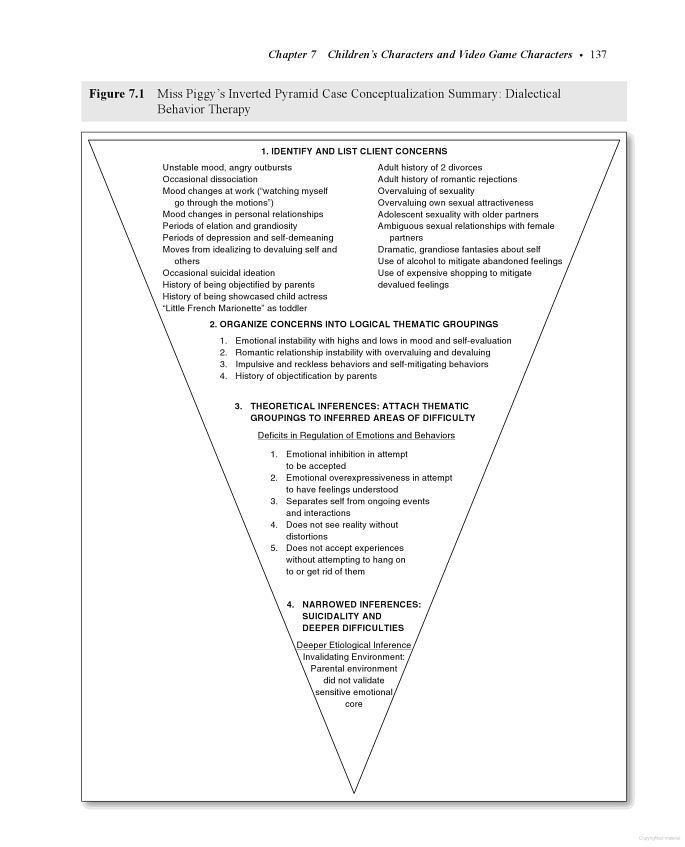
Why is it important to involve clients in case conceptualization and treatment planning?
Hays notes that involving clients in case conceptualization and treatment planning also allows for better cultural understanding and responsiveness. Counselors have a significant responsibility to get a client’s story right, she says, and “getting the story right involves co-constructing it with the client in a way that honors their cultural experiences as well as points of trauma and resilience.”
What is the most integrative and effective way to devise a rich treatment plan?
Practically applying that knowledge is “where the rubber hits the road,” says Ivers, a member of the American Counseling Association. Examining a client’s concerns in depth — moving beyond surface-level questions such as “How did this week go?” or “What do you want to talk about?” — is the most integrative and effective way to devise a rich treatment plan and pinpoint a destination that the client and practitioner will work toward together in therapy.
How to stay informed in counseling?
Karl urges clinicians to stay informed and up to date by attending workshops, conferences and other continuing education events; consulting regularly with professional peers; seeking mentorship or supervision; joining professional Listservs; and reading counseling journals and other publications. Remaining active with state and local counseling organizations will also help practitioners stay abreast of criteria and processes that vary state to state, she notes. Leadership within the counseling profession must ensure that funding for continuing education on assessment, diagnosis and treatment planning is prioritized, especially for counselors in economically disadvantaged or rural areas and settings where practices or clinics are short-staffed, Karl adds.
Why is diagnosis important to Keller?
Diagnosis is a tool that allows her to understand how she can initially help her clients, and it guides her interventions and therapeutic approach as treatment progresses. It can also remove financial barriers to mental health care. Counseling can be expensive, and insurance companies typically require a diagnosis for reimbursement. So, Keller views diagnosis as a way of providing treatment access for clients who wouldn’t be able to afford counseling without insurance coverage.
What is Keller's key to psychoeducation?
The key, Keller says, is to be fully transparent with clients and include them in the diagnostic process, especially for diagnoses that can carry a stigma, such as personality disorders, substance use disorders and eating disorders. In some cases, counselors may need to offer psychoeducation to dispel inaccuracies or stereotypes about a diagnosis.
What is the core of professional counseling?
Fully understanding a client’s situation, symptoms and needs and then matching them with a diagnosis (when appropriate) and a treatment plan that will help them heal, grow and thrive are core aspects of professional counseling. Counselors learn these skills, at least conceptually, in graduate school but gain true understanding of them through their direct work with clients.
How to help clients with eating disorders?
Clients presenting with symptoms of an eating disorder might respond with statements such as “I don’t want to fight my body anymore” or “I’m sick of hating my body,” Keller says. In this example, Keller and the client might work together to create a goal of improving the client’s body image in counseling. Later, once the client has made some progress on that goal and established a stronger therapeutic relationship with Keller, she will circle back to some of the issues that revealed themselves in the initial assessment session and try to tie those issues into the client’s treatment goals. If the client mentioned purging behavior or restrictive eating in the initial session, for example, Keller might gently raise the idea that this behavior could be something to work on as part of reaching the client’s goal of obtaining a healthy body image.
What is a plan of services?
For beneficiaries receiving mental health or developmental disabilities services, the individual plan of services must be developed through a person-centered planning process
What is the goal of the drug problem?
Problem: “Using drugs has caused too many problems in my life.” Goal #1: “I want to stop using drugs and figure out how not to relapse anymore”Objective #1: Write a detailed chemical use history describing treatment attempts and the specific situations surrounding relapse.