The tooth chart reveals this information quickly and concisely in outline form. Include a sheet with a diagram of all teeth. Existing restorations should be indicated in blue pencil and work that needs to be done in red pencil.
Full Answer
Why is the patient chart important in dentistry?
The patient chart is also a means of communication between the treating practitioner and other clinicians who may treat that patient in the future. Thus, the dental record should contain enough information to allow another provider to understand the patient’s experience in your office. What should the dental record contain?
What should be included in a patient chart?
The patient chart must likewise include a notation of any significant dental history, e.g. an assessment of caries risk and periodontal health. Every patient is unique and the dental history should be considered together with the clinical examination when planning and sequencing of dental care.
How are dental treatment procedures annotated on the dental chart?
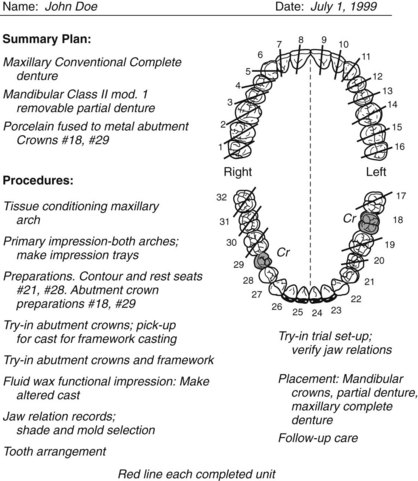
On approval, treatment procedures are performed and annotated on the dental chart (Figs. 6–8). A. Occlusal adjustment reductions are re- corded on the dental diagram by shading in the portion of each tooth that has been removed and describing the procedure in the treatment section of the chart.
What should be included in a dental treatment note?
Treatment notes give us the details of a procedure. The tooth chart reveals this information quickly and concisely in outline form. Include a sheet with a diagram of all teeth. Existing restorations should be indicated in blue pencil and work that needs to be done in red pencil.

How do you write dental records?
Information typically noted in the dental record includes:personal data, such as the patient's name, birth date, address and contact information including home, work and mobile telephone numbers.the patient's place of employment.medical and dental histories, notes and updates.progress and treatment notes.More items...
How do you present a dental treatment plan?
2:556:26How to present dental treatment plans and why this ... - YouTubeYouTubeStart of suggested clipEnd of suggested clipWe're presenting treatment to the patients on their way out of the front door like they just got outMoreWe're presenting treatment to the patients on their way out of the front door like they just got out of the chair that bibs off and they're mine the appointments over we bring them to the front desk.
What is included in a dental chart?
Dental records, also known as patient charts, are made up of the recorded information regarding your medical history, diagnostic information, clinical notes, patient-doctor communication, consent to treatment documents and treatment notes, as the American Dental Association (ADA) explains.
How do you use a dental chart?
0:4715:13Dental Charting Procedures - YouTubeYouTubeStart of suggested clipEnd of suggested clipOr black penciled X is placed over all surfaces of the tooth on the chart. Open contact areas areMoreOr black penciled X is placed over all surfaces of the tooth on the chart. Open contact areas are designated by grey or black parallel lines placed between the two teeth.
What is a treatment presentation?
The first step in a treatment presentation (in particular, an elective one) is to evaluate the patient's motivation level. Once the patient has demonstrated interest, you can then create excitement by offering an enthusiastic presentation that will help the patient recognize the benefits of treatment.
When is a treatment plan presented to the patient in dentistry?
It is during the sequencing stage that a dentist will flex their ability to handle complex issues and distill them into a comprehensive plan of action. To organize the stages into a proper sequence of treatments, a dentist should: Review the stages and the different treatments they plan to use.
What is an example of an important record in a dental office?
Useful records include employment applications, expired insurance policies, petty cash vouchers, bank reconciliations, and general correspondence. This category is difficult to define, because one office may consider a document useful, whereas another might find it indispensable.
What are the different types of dental charting?
The three most common systems are the FDI World Dental Federation notation (ISO 3950), the Universal Numbering System, and the Palmer notation. The FDI notation is used worldwide, and the Universal is used widely in the United States. The FDI notation can be easily adapted to computerized charting.
What should not be included in a patient medical record?
The following is a list of items you should not include in the medical entry:Financial or health insurance information,Subjective opinions,Speculations,Blame of others or self-doubt,Legal information such as narratives provided to your professional liability carrier or correspondence with your defense attorney,More items...•
How do I read a perio chart?
The Meanings of the Measurements0-3mm without bleeding: Perfect! ... 1-3mm with bleeding: Early signs of gingivitis. ... 3-5mm with no bleeding: This is an indication that there is a potential for gum disease. ... 3-5mm with bleeding: This is an early stage of gum disease or the beginning of periodontitis.More items...•
What does TX mean in dental terms?
Tx – Treatment. UL – Upper left quadrant. Also called Quadrant 2.
How do you record on BPE?
BPE should be used for screening only and should not be used for diagnosis. To record an adult's BPE, the dentition should be divided into six sextants – upper right, upper anterior, upper left, lower right, lower anterior and lower left – and the highest score for each recorded.
What percentage of dental charts are computerized?
2. Legible — Amazingly, only 36 percent of American dental offices are computerized. The majority of charts are handwritten.
What percentage of Americans have periodontal disease?
Perio chart — According to the ADA, more than 75 percent of American adults have some form of periodontal disease — the major cause of adult tooth loss in the United States. Research is now showing a correlation between periodontal disease and heart disease.
What are the advantages of AADD?
Advantages are reduced filing time by 50-80 percent, eliminated misfiling, and automatic chart audit. The letters AADD don't represent anything. The AADD system represents efficiency at its best. For more information about the system, visit the Web site at www.aads-filing.com.
What should be included in a dental hygiene note?
A dental hygiene note should include: Medical history. Review and update it, noting any changes (medications, allergies, surgeries, medical conditions, etc.). If a patient reports no changes in their medical history, state, “Patient reports no changes” in your notes. Intraoral/extraoral cancer exam.
Why is chart note important?
Chart notes are considered legal documents and, according to the American Dental Association, are “critical in the event of a malpractice insurance claim.” 1 The notes keep track of the procedures, treatments, recommendations, and findings from previous dental visits.
Patient record
The patient record is the history of your therapeutic relationship with your patient. It gives you all of the information you need to continue treating that patient appropriately. Complete records should include:
Health history
Make sure to note any conditions requiring premedication, history of infectious disease or illness, allergies and any tobacco, drug or alcohol usage.
Medications
Document any medications given, recommended or prescribed in the record. Documentation of complete prescription information should include:
Treatment Information
Note examples of pertinent information include the patient’s current dental complaint, current oral condition by examination and radiograph findings.
Treatment planning
Before initiating any treatment, the patient record should reflect a diagnosis of the patient’s problem based on the clinical exam findings and the medical and dental histories.
Oral cancer screening
As part of every patient’s oral exam appointment, perform an oral cancer screening. Inspect the head, neck, lips, floor of the mouth, front and sides of the tongue and soft and hard palates.
Periodontal probing
The evaluation and documentation of a patient’s periodontal health is part of the comprehensive dental examination. Current standards call for full-mouth periodontal probing at each hygiene recall visit, and the absence of that information in the chart might be construed as failure to conduct the periodontal examination.
Why is a dental record important?
Beyond patient care, the dental record is important because it may be used as evidence in court or in a regulatory action to establish the diagnostic analysis that was performed and what treatment was rendered to the patient.
How long do you have to keep dental records?
How long do we have to keep dental records? In general, clinical and financial records, as well as radiographs, consultation reports, and drug and lab prescriptions must be maintained for at least ten years after the date of the last entry in the patient’s record.
Why is it important to record patient information?
The dental record (aka patient chart) is the official source of all diagnostic information, clinical notes, treatment and patient-related communications that occur in the dental office, including instructions for home care, consent to treatment and finances. It provides invaluable data, which can be used to assess the quality of care that has been provided and to properly plan for treatment going forward.
What happens if a chart doesn't justify the claim submitted?
by insurance companies). If the chart doesn’t justify the claim submitted, an insurance company might refuse payment or demand reimbursement. This will certainly lead to an upset patient, and if there is a serious discrepancy between the progress notes and the bill submitted, fraud might be suspected. In these situations, insurance companies could audit your records or even report you to the College. Keeping good records helps avoid this unnecessary stress. For example:
Do electronic records leave an audit trail?
Electronic records must leave an audit trail that accomplishes the same result. Late entries should be clearly marked as such. In no circumstances should a clinician add to or correct a patient’s chart after receiving a demand for compensation or notice of legal proceedings.
When should progress notes be completed?
Because they are essential for treatment continuity, progress notes should be completed during or immediately after each visit and must be reviewed and approved by the treating clinician.
Can Zirconoia crown be retroactively altered?
If you provide a Zirconoia crown and accidentally submit the code for a PFM, you might be accused of insurance fraud or overbilling. Never, never retroactively alter the patient chart. To avoid allegations of tampering, errors or incorrect information should never be erased or eliminated from the chart.
What is a dental chart template?
Dental chart templates are used by dental healthcare professionals to describe the condition of your teeth and gums. You can find here a dental chart template or perio chart templates available in PDF and DOC formats. Dental care is very important for humans and pet animals like dogs and cats, you can understand the condition of the teeth with the dental teeth chart template. Browse our collection to find the best one that helps you to understand the health of your teeth and gums.
Why do dentists use dental charts?
It is used by dental healthcare professionals to explain the patient about their teeth condition because a common person doesn’t understand the dental terms. Dental charts are usually done when you have some dental issues and visit your dentist. Baby dental teeth chart is done when your baby starts teething and parents want to understand ...
What are the benefits of dental charts?
There are significant benefits of dental charts, you can get all these advantages with our awesome collection of dental chart templates with symbols. Some benefits of dental chart are as follows: 1 It helps to state a clear description of your dental conditions. 2 Work as your medical record 3 Help the dentist to give you better treatment 4 Easily to use and understand the condition of your teeth and gums 5 Help to identify your dental problem easily 6 Graphics helps you to understand it easily and efficiently 7 Best way to track your dental progress
What is the best way to understand the condition of your teeth and gums?
Graphical representation of your teeth is the best way to understand the condition of your teeth and gums. It includes every tooth of your mouth with space, cavity indication symbols, missing teeth and other related information of your teeth.
What information is needed to identify each tooth?
The typical things must be included in the dental chart are as follows: Patient’s name, gender and contact information. Medical and dental history. Specific information about the health of your teeth.
Why is a dental chart important?
To keep your dental information, a dental chart is the best way to organize and save it for future use.
Can you access your medical records?
Medical records are not accessible by every person, patient or their parents issuing a medical release form to access the patient’s medical record or history. If you have some dental issues in the future then this dental chart is used to tell the doctor about your medical record.
Oral lesions: Gathering evidence
Crafting written descriptions of oral lesions is like recording evidence from a crime scene: it's important to gather as many clues as possible. The clues we find will guide us to the right action, be it monitoring the situation, gathering additional information, or referring patients to a specialist.
Eight steps of documentation
Here are the eight steps to describing and recording clinical findings for oral lesions.
Memory tricks
To remember the eight components, you can use a memory technique that I teach at WakeUp Memory and my RDH Under One Roof presentation on oral pathology. In this case, you make an acronym of the first letter for each component: LDSSCCTH. Now, make a sentence (or sentences) that you can remember. Here are examples of ones that help me:
Documenting details
Knowing the eight steps is a good start, but let’s look at each item closer. This will help you become proficient in charting oral lesions accurately.
Differential diagnosis
After you complete the eight-step oral lesion charting, then you can start formulating a differential diagnosis. You can also ask for the help of the doctor or a specialist. Remember: documentation can save your patient's life!
Practice
Here is a practice image in Figure 2. Try to describe it using the eight components of good oral lesion descriptions. For this example, take a guess the consistency and texture. (This is only for practice!)
Resources
DeLong L., Burkhart NW. General and oral pathology for the dental hygienist. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins, 2013.
How many pages should a dental treatment plan be?
You can include a second page for Payment Schedule / Financial arrangement only – but a treatment plan should be one page. Include area of the mouth: when writing out recommended treatment on the plan, don’t just list teeth numbers.
When writing out recommended treatment on the plan, what should you include?
Include area of the mouth: when writing out recommended treatment on the plan, don’t just list teeth numbers . Patient doesn’t know teeth numbers, they may remember what you told them during the exam if you write out where the tooth is located in their mouth .
Do you need to have built trust with patients before a bridge?
Let’s dive right in. Just because you’re starting out, don’t think you won’t get a patient right away in the door who needs a bridge, implants, multiple endos, etc. It’s true that for majority of the patients, you need to have built trust with them prior to you providing any treatment for them.
What is included in a dental record?
The following are examples of what is typically included in the dental record 1: 1 Patient’s personal database, such as name, birth date, address, and contact information, place of employment and telephone numbers (home, work, mobile) 2 Medical and dental histories, notes, and updates 3 Progress and treatment notes 4 Conversations about proposed treatment, the potential benefits and risks, and alternatives associated with that treatment.
What is the dental record?
According to the American Dental Association, “The dental record also serves to provide continuity of care for the patient and is critical in the event of a malpractice insurance claim,” and the “information in the dental record should primarily be clinical in nature.”. The following are examples of what is typically included in the dental record 1:
Is it okay to quote a patient's words?
Quoting a patient’s words, in quotations and accurately – is perfectly okay. Objectively stating something the patient may have done, such as arrived late, requested something specific, declined a recommendation, moved during an injection – is also okay.
Can a note be removed from a medical record?
An addendum, or comment of correction, can likely be made, but a note cannot be removed once it is part of the record . 2. As healthcare professionals, we should follow the lead of other medical professionals when it comes to our record keeping.
Can a dental board subpoena a dental record?
Dental records in their entirety are often subpoenaed by lawyers for a plethora of reasons or can be requested by the dental board , perhaps if a patient has filed a complaint. In this case, it is often required an exact, duplicate copy of records sent to the presiding dental board is to be sent to the patient.
What is a dental chart?
The dental chart is a legal document. It is the first line of defense in a malpractice suit. When a patient decides to file a lawsuit against a dentist, the dental chart becomes the single most important piece of information relative to the suit.
What is thorough documentation?
Thorough documentation includes the complete and accurate recording of all collected data, treatment planned and provided, recommendations, and other information relevant to patient care and treatment.
How often should a patient's medical history be updated?
The medical history should be updated at every patient visit by the clinician. At least once per year, the patient should be asked to verify that his or her current medical history is correct by signing the form (or tablet in paperless offices).
Can incomplete dental records be damaging?
People get sloppy with record-keeping. The fact is that in a court of law or before a state dental board, incomplete records could prove to be the most damaging factor to the clinician. Remember that in the eyes of the law or a state dental board, if something is not recorded in the chart, it never happened.