What drugs are used to treat TB?
1. Garlic...
2. Bananas...
3. Drumstick...
4. Indian Gooseberry...
5. Oranges...
6. Custard Apple...
7. Black Pepper...
8. Walnuts...
Learn More...What are the side effects of TB medications?
These are the three treatment options:
- Isoniazid (INH): This is the most common therapy for latent TB. You typically take an isoniazid antibiotic pill daily for 9 months.
- Rifampin ( Rifadin, Rimactane): You take this antibiotic each day for 4 months. ...
- Isoniazid and rifapentine: You take both of these antibiotics once a week for 3 months under your doctor’s supervision.
Is MDR TB curable?
When taking these medications, call your doctor immediately if you have any of the following:
- Nausea or vomiting
- Loss of appetite
- A yellow color to your skin (jaundice)
- Dark urine
- Easy bruising or bleeding
- Blurred vision
What is the treatment for drug resistant TB?
Treatment of MDR-TB. It is curable but has long term hazards on the body. Yes, it is 100% curable. Multi-drug resistance tuberculosis is TB that does not respond to at least rifampicin and isoniazid, the two powerful anti-tb drugs.

WHO guidelines MDR-TB treatment?
Current policy recommendations on treatment and care for DR-TB. In patients with confirmed rifampicin-susceptible and isoniazid-resistant tuberculosis, treatment with rifampicin, ethambutol, pyrazinamide and levofloxacin is recommended for a duration of 6 months.
How MDR-TB is treated?
Levofloxacin and moxifloxacin are the two most frequently recommended agents, and the WHO has recommended the use of these drugs for the treatment of MDR-TB. The optimal dose of levofloxacin is 750 mg once daily and that of moxifloxacin is 400 mg once daily.
WHO recommended TB treatment?
For treatment of new cases of pulmonary or extrapulmonary TB, WHO recommends a standardized regimen consisting of two phases. The initial (intensive) phase uses four drugs (rifampicin, isoniazid, pyrazinamide and ethambutol) administered for two months.
Can MDR-TB be cured completely?
The Grim Facts of Today's TB Therapy The pandemic can't be overcome without improved cures. Only about half the people with MDR-TB around the world are successfully cured. TB treatment is lengthy and burdensome to patients and treatment providers alike.
How long is MDR treatment?
MDR- and XDR-TB need prolonged treatment duration, from 18 to 24 months after sputum culture conversion, as recommended by the World Health Organization (WHO) [2]. A prolonged duration of treatment may lead to poor adherence, higher cost and undue toxicity.
How is MDR treated and how long is the treatment?
The recommended dose of bedaquiline for the treatment of pulmonary MDR in adults is: Weeks 1 – 2: 400 mg (4 tablets of 100 mg) given orally, once daily. Weeks 3 – 24: 200 mg (2 tablets of 100 mg) three times per week, for a total dose of 600 mg per week.
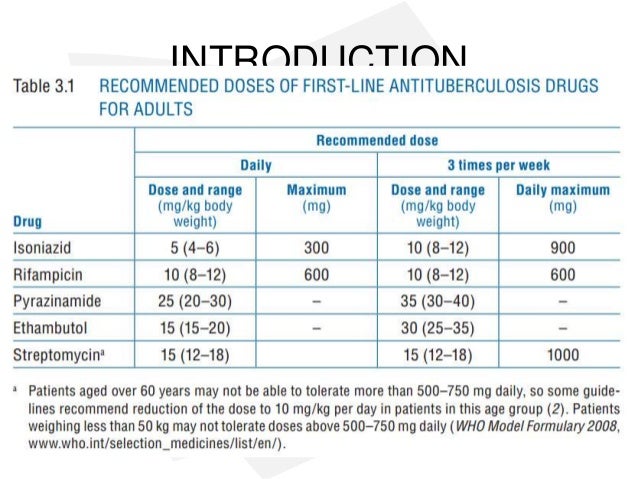
What is first-line treatment for TB?
Of the approved drugs, isoniazid (INH), rifampin (RIF), ethambutol (EMB), and pyrazinamide (PZA) are considered first-line anti-TB drugs and form the core of standard treatment regimens (Figure 6.4) (Table 6.2).
What is the first-line drug for TB?
First-line agents for treatment of active TB consist of isoniazid, a rifamycin (rifampin or [less frequently] either rifapentine or rifabutin), pyrazinamide, and ethambutol; in addition, moxifloxacin is a first-line agent when administered in combination with isoniazid, rifapentine, and pyrazinamide [6].
What is the second line treatment of TB?
Grouping of drugsDrugs line categoryGroup 1Isoniazid, rifampicin, ethambutol, pyrazinamideSecond-line anti-tuberculosis drugsGroup 2Moxifloxacin, high dose levofloxacin (fluoroquinolones)Group 3Linezolid, delamanid, bedaquiline (newer drugs with increased evidence)4 more rows•Oct 14, 2016
How long does MDR-TB patient live?
MDR-TB incidence exceeds 70 cases per 100,000 population and a recent study found that the median time to death for MDR- and XDR-TB, respectively, was 60 days and 28.5 days.
Is MTB curable?
Tuberculosis, also known as TB, is an airbone infectious disease caused by the bacteriumMycobacterium tuberculosis that is preventable and curable.
How serious is MDR-TB?
MDR-TB, which is deemed a public health crisis by the World Health Organization (WHO), is caused by strains of TB bacteria that do not respond to standard antibiotics, which can lead to treatment failures or death.
What is the most effective anti-TB drug?
Fluoroquinolones are often the most effective anti-TB drugs in an MDR-TB regimen. There are two important recommendations regarding fluoroquinolone use from the 2011 update of the Guidelines for the programmatic management of drug-resistant tuberculosis(1).
How early can you start anti-TB treatment?
Antiretroviral therapy (ART) is recommended for all patients with HIV and drug-resistant TB, irrespective of CD4 cell-count, as early as possible (within the first eight weeks) following initiation of the anti-TB treatment (strong recommendation) (1). The drug dosage is usually determined by age and weight.
Does Linezolid work for meningitis?
Linezolid is believed to penetrate the central nervous system, and has been used in meningitis treatment (35). Imipenem has good central nervous system penetration, but children with meningitis treated with imipenem, had high rates of seizures (meropenem is preferred for meningitis cases and children) (11,36,37). 5.12.
What is MDR TB?
What is multidrug-resistant tuberculosis (MDR TB)? Multidrug-resistant TB (MDR TB) is caused by an organism that is resistant to at least isoniazid and rifampin, the two most potent TB drugs. These drugs are used to treat all persons with TB disease.
How to prevent MDR TB?
Another way to prevent getting MDR TB is to avoid exposure to known MDR TB patients in closed or crowded places such as hospitals, prisons, or homeless shelters. If you work in hospitals or health-care settings where TB patients are likely to be seen, you should consult infection control or occupational health experts.
Why is XDR TB so resistant to TB drugs?
Because XDR TB is resistant to the most potent TB drugs, patients are left with treatment options that are much less effective. XDR TB is of special concern for persons with HIV infection or other conditions that can weaken the immune system.
What are the symptoms of TB in the lungs?
The symptoms of TB disease of the lungs may also include coughing, chest pain, and coughing up blood. Symptoms of TB disease in other parts of the body depend on the area affected. If you have these symptoms, you should contact your doctor or local health department.
What to do if you think you have been exposed to someone with TB?
If you think you have been exposed to someone with TB disease, you should contact your doctor or local health department about getting a TB skin test or TB blood test. And tell the doctor or nurse when you spent time with this person.
Can TB be curable?
TB usually affects the lungs, but it can also affect other parts of the body, such as the brain, the kidneys, or the spine. In most cases, TB is treatable and curable; however, persons with TB can die if they do not get proper treatment.
What is MDR TB?
Multidrug-resistant tuberculosis (MDR-TB) is an increasing global problem, with most cases arising from a mixture of physician error and patient non-compliance during treatment of susceptible TB. The extent and burden of MDR-TB varies significantly from country to country and region to region. As with TB itself, the overwhelming burden of MDR-TB is in high-burden resource-poor countries. The diagnosis depends on confirming the drug susceptibility pattern of isolated organisms, which is often only possible in resource-rich settings. There should be a strong suspicion of drug resistance, including MDR-TB, in persons with a history of prior treatment or in treatment failure cases. Treatment in developed countries is expensive and involves an individualized regimen based on drug susceptibility data and use of reserve drugs. In resource-poor settings a WHO retreatment regimen may be used, but increasingly the move is to a directly observed treatment based 'DOTS-plus' regimen in a supported national TB programme. However, even where such treatment is given, the outcome for patients is significantly worse than that for fully susceptible TB and has a much higher cost.
What is treatment in developed countries?
Treatment in developed countries is expensive and involves an individualized regimen based on drug susceptibility data and use of reserve drugs.