What are some treatment options for someone who is suffering from alcoholism?
Options for TreatmentBehavioral Treatments. Behavioral treatments are aimed at changing drinking behavior through counseling. ... Medications. ... Mutual-Support Groups. ... Current NIAAA Research—Leading to Future Breakthroughs. ... Mental Health Issues and Alcohol Use Disorder.
What is the most effective treatment for alcohol dependence?
Naltrexone (Trexan) and acamprosate (Campral) are recommended as FDA-approved options for treatment of alcohol dependence in conjunction with behavior therapy.
Which medication has a greater advantage for treatment of alcohol withdrawal syndrome?
Benzodiazepines have the largest and the best evidence base in the treatment of alcohol withdrawal, and are considered the gold standard. Others, such as anticonvulsants, barbiturates, adrenergic drugs, and GABA agonists have been tried and have evidence.
What are 3 medications that can be used for alcohol dependence?
Medications Used to Treat AlcoholismCOMBINE Study.Antabuse (Disulfiram)Naltrexone.Campral (Acamprosate)The Sinclair Method.
What drug is commonly used to treat alcoholics?
Three medications are approved by the U.S. Food and Drug Administration to treat alcohol use disorder: acamprosate, disulfiram, and naltrexone. Acamprosate and naltrexone reduce alcohol consumption and increase abstinence rates, although the effects appear to be modest.
What is naltrexone HCL used for?
Naltrexone is used to help narcotic dependents who have stopped taking narcotics to stay drug-free. It is also used to help alcoholics stay alcohol-free. The medicine is not a cure for addiction.
Why do we give thiamine to alcoholics?
Thiamine supplementation reduces the risk of developing Wernicke syndrome, Korsakoff syndrome, and beriberi. Physicians working with patients with alcohol use disorders should have a high index of suspicion for Wernicke syndrome, particularly if the patient shows evidence of ophthalmoplegia, ataxia, or confusion.
Why do alcoholics need folic acid?
An important mechanism in alcohol-induced injury is biomolecular oxidative damage. Folic acid is supplied to chronic alcoholic patients in order to prevent this situation, as this is the main vitamin deficiency that they suffer from.
How does naltrexone work for alcohol dependence?
Naltrexone blocks the parts of your brain that “feel” pleasure from alcohol and narcotics. When these areas of the brain are blocked, you feel less need to drink alcohol, and you can stop drinking more easily.
What is the best antidepressant for alcoholics?
The antidepressants nefazodone, desipramine, and imipramine were found to have the most robust effects on decreasing depressive symptoms.
Is Flagyl used to treat alcoholism?
Metronidazole ('Flagyl') has recently been said to be of value in treating alcoholism (Taylor, 1964). The drug is, of course, better known for its use against trichomoniasis.
What is used for pharmacologic management of alcohol dependence?
Pharmacologic Therapy The ultimate goals for patients with alcohol dependence are to achieve abstinence and prevent relapse. Currently, the four pharmacologic agents that may aid in accomplishing these goals are disulfiram, oral naltrexone, injectable extended-release naltrexone, and acamprosate.
When Drinking Becomes Alcoholism
Worldwide alcohol use and abuse statistics are staggering. The single highest risk factor for premature death and disability for individuals between 15 and 49 years old across the world is alcohol abuse. 1 In the United States, 1 in 10 children live ...
The Effects of Alcohol Use
Moderate Drinking vs. Alcohol Abuse It's true that many sources point to the health benefits of moderate alcohol consumption. The key word here is moderate. Some studies have shown a connection between light to moderate drinking and decreased heart ...
Concurrent Alcohol and Norco Abuse
Norco, which is the brand name for hydrocodone is a narcotic pain reliever. If you are misusing Norco, your body may be dependent on the drug, ultimately resulting in addiction. Concurrent alcohol and Norco abuse occurs when someone is using both ...
Alcohol and Breastfeeding
Many women are curious about whether they can drink alcohol while they are breastfeeding. While women are strongly advised to avoid drinking any alcohol during pregnancy , the recommendations on whether a woman can drink while breastfeeding are less ...
Alcohol Abuse Prevention
Given the prevalence of alcohol abuse in the adult population, it makes sense that we should focus on early prevention efforts aimed at young people. In today's world, kids are subjected to a number of societal pressures—from advertising, ...
Alcohol: The Breast Cancer Risk in a Bottle
Can drinking alcohol cause breast cancer? That's the question multiple experts, research teams, scientists, and medical oncologists have set out to answer. And what they've found might surprise you. When most people think about the adverse effects ...
12-Step Thinking: Let's Talk About AA and the C-Word (Uncovering Alcoholics Anonymous)
No, not that c-word! To be clear, we're talking about the word cult here. If you're familiar with the world of addiction recovery, then you're no doubt acquainted with Alcoholics Anonymous—or AA as it is more commonly known. And if you've had more ...
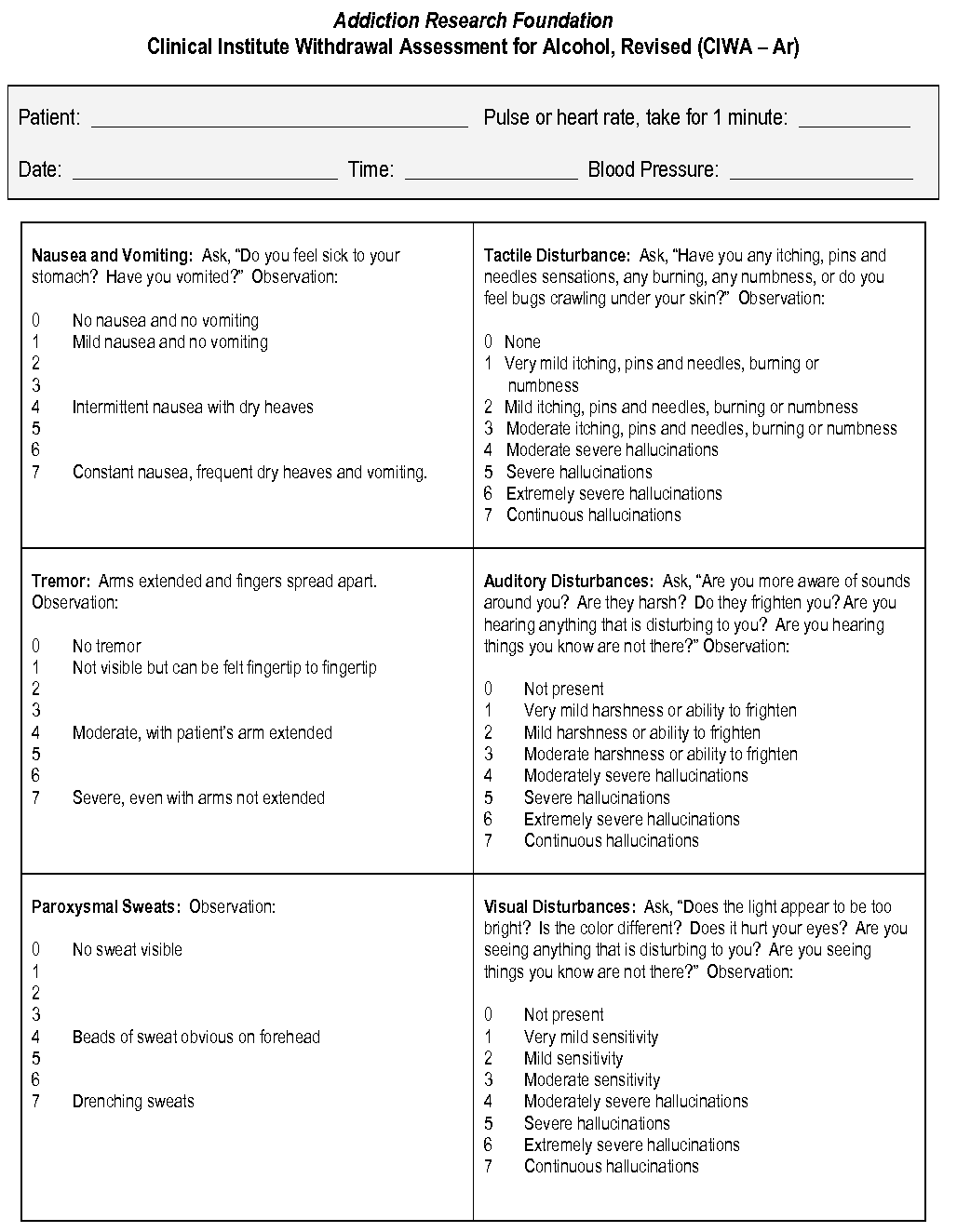
What is the ASAM risk assessment matrix?
Recommendation III.3:The ASAM Criteria Risk Assessment Matrix and withdrawal severity scales can be helpful for determining the appropriate level of care for managing patients in alcohol withdrawal. Most withdrawal severity scales reflect current signs and symptoms and should not be used alone to determine level of care.
How many levels of care are there for withdrawal management?
While there are five distinct levels of care for withdrawal management defined by The ASAM Criteria, much of the research on patient placement evaluates factors indicating (or contraindicating) placement in an ambulatory or inpatient treatment setting. These settings align with the following ASAM levels of care:
How are ASAM recommendations drafted?
Recommendations were drafted by the project team by combining the statements identified as clinically appropriate by the Guideline Committee. Recommendations are accompanied by a brief discussion of the evidence or rationale for the statement. ASAM's two prior alcohol withdrawal guidelines were used as an initial framework for the guideline. This first draft of the guideline was reviewed by the Clinical Champions, Guideline Committee Moderator and Guideline Committee Members to ensure content clarity and logical flow of the guideline. A second draft was produced based on this feedback.
How long to check in with a qualified health provider?
Recommendation IV.1: In ambulatory settings, arrange for patients to check in with a qualified health provider (e.g., medical assistant, nurse) daily for up to five days following cessation of (or reduction in) alcohol use. For some patients who are unable to attend daily in-person check-ins, alternating in-person visits with remote check-ins via phone or video call is an appropriate alternative.
What is the practice guideline for alcohol withdrawal?
The American Society of Addiction Medicine (ASAM) developed this Guideline on Alcohol Withdrawal Management to provide updated information on evidence-based strategies (hereafter referred to as the Practice Guideline) and standards of care for alcohol withdrawal management in both ambulatory and inpatient settings.
When feasible, alcohol use disorder (AUD) treatment should be initiated concurrently with alcohol withdrawal management as cognitive status permits?
Recommendation IV.12: When feasible, alcohol use disorder (AUD) treatment should be initiated concurrently with alcohol withdrawal management as cognitive status permits. If appropriate, clinicians should offer to initiate pharmacotherapy for AUD as cognitive status permits. If not initiating AUD treatment themselves, clinicians should explain the range of evidence-based treatment services available in the community, and engage patients with these options. In addition, clinicians may offer information about local recovery support groups, including 12-step groups.
What is the DSM 5?
Recommendation I.5: To diagnose alcohol withdrawal and alcohol withdrawal delirium, use diagnostic criteria such as those provided by the Diagnostic and Statistical Manual 5 (DSM-5). To diagnose alcohol use disorder, use diagnostic criteria such as those provided by the DSM-5.
How to develop a comprehensive practice guideline focused on alcohol withdrawal management?
In order to develop a comprehensive practice guideline focused on alcohol withdrawal management, we utilized a hybrid of established methodologies. In order to develop the scope of the guideline and draft the guideline statements, we followed the Veterans Health Administration and Department of Defense (VA/DoD) Guideline for Guidelines. To rate and refine the draft guidelines, we used the RAND/UCLA Appro- priateness Method (RAM), which is a specific process for combining the available scientific evidence with the clinical judgment of experts. Quality of the literature reviewed was rated using standardized rating scales and methodology. The external review process was informed by the VA/DoD method.
How often should alcohol withdrawal management be updated?
Second, updated QIC policies recommend that all ASAM guidelines should be updated every five years. ASAM’s previous guidelines on the topic of alcohol withdrawal management were published in 1997 and2004. The first guideline, ‘‘Pharmacological Management of Alcohol Withdrawal’’13was published in JAMA, followed five years later with the most recent guideline entitled ‘‘Management of Alcohol Withdrawal Delirium’’14in JAMA Internal Medicine, formerly Archives of Internal Medicine. Subsequent guidelines have not been written since the 2004 guidelines thus an update was due. Third, the American Psychiatric Association (APA) released a practice guideline in 2018 on the appropriate use of medications in the treatment of alcohol use disorder that is not inclusive of alcohol withdrawal management.15An ASAM guideline on alcohol withdrawal should complement APA’s guideline to provide clinicians with guidance on treatment and management approaches across a continuum of care. Fourth, outreach to other organizations indicated that other organizations are not planning on creating a guideline on alcohol withdrawal management.
What factors increase the risk of complications of withdrawal?
RecommendationII.5:Assess for the following factors associated with increased patient risk for complicated with- drawal or complications of withdrawal: History of alcohol withdrawal delirium or alcohol with- drawal seizure Numerouspriorwithdrawalepisodesinthepatient’slifetime Comorbid medical or surgical illness (especially traumatic brain injury) Increased age (>65) Long duration of heavy and regular alcohol consumption Seizure(s) during the current withdrawal episode Marked autonomic hyperactivity on presentation Physiological dependence on GABAergic agents such as benzodiazepines or barbiturates Recommendation II.6: The following individual fac- tors may increase a patient’s risk for complicated withdrawal or complications of withdrawal: Concomitant use of other addictive substances Positive blood alcohol concentration in the presence of signs and symptoms of withdrawal Signs or symptoms of a co-occurring psychiatric disorder are active and reflect a moderate level of severity Recommendation II.7: Patients’ risk for complicated withdrawal or complications of withdrawal is increased by the presence of multiple risk factors. Recommendation II.8: In general, clinicians may con- sider patients at risk of severe or complicated withdrawal if
What is withdrawal management?
Withdrawal Management: This term has replaced the formerly used ‘‘detoxification.’’ Withdrawal management refers to the medical and psychological care of patients who are experiencing withdrawal symptoms as a result of ceasing or reducing their substance use. 11The process of withdrawal management includes not only attenuation of the physiological and psychological features of withdrawal, but also interrupting the momentum of habitual compulsive use in persons with SUD.12
What is considered unhealthy alcohol use?
Unhealthyalcoholuse:Includes the following patterns of alcohol use: 1) Binge drinking (defined as consuming 4 or more alcoholic beverages per occasion for women or 5 or more drinks per occasion for men); 2) Heavy drinking (defined as consuming 8 or more alcoholic beverages per week for women or 15 or more alcoholic beverages per week for men ); 3) Any drinking by pregnant women or those younger than age 21.10
What is a treatment plan?
Treatmentplan:A therapeutic strategy that may incor- porate patient education, drug therapy, and the participation of health professionals. Treatment plans are especially important in the optimal management of complex or chronic illnesses such as SUDs.3
What is a substance use disorder?
Substance Use Disorder (SUD): Substance use disor- der is marked by a cluster of cognitive, behavioral, and physiological symptoms indicating that the individual con- tinues to use alcohol, nicotine, and/or other drugs despite significant related problems . Diagnostic criteria are given in the DSM-5. Substance use disorder is the new nomenclature for what was included as substance dependence and substance abuse in the DSM-4.