While vitamin supplementation can be useful for other health conditions, do provide not Vitamins C, D, or E, to pregnant women as part of a strategy for prevention of PE/E. Low-dose acetylsalicylic acid (aspirin, 75 mg) for the prevention of pre-eclampsia in women at high risk of developing the condition. Individual or combined vitamin C and vitamin E supplementation. Antihypertensive drugs for pregnant women with severe hypertension. Use of diuretics, particularly thiazides, for prevention of pre-eclampsia and its complications.
Full Answer
What are the treatment options for preeclampsia?
If a patient has an elevated blood pressure reading, the reading should be confirmed with repeated measurements. Management strategies for diagnosed preeclampsia may include close fetal and maternal monitoring, antihypertension medications, and magnesium sulfate.
Is pre-eclampsia avoidable?
WHO Recommendations for Prevention and Treatment of Pre-Eclampsia and Eclampsia The majority of deaths due to pre-eclampsia and eclampsia are avoidable through the provision of timely and effective care to the women presenting with these complications.
How are antihypertension medications used to treat eclampsia?
Antihypertension medications, when indicated, and administration of magnesium sulfate reduce the risk of adverse events. The Magpie Trial (n=10,141), an international randomized clinical trial of treatment with magnesium sulfate, showed a benefit for preventing eclampsia.
What are the clinical conditions associated with increased risk of preeclampsia?
Important clinical conditions associated with increased risk include a history of eclampsia or preeclampsia (particularly early-onset preeclampsia), previous adverse pregnancy outcome, maternal comorbid conditions (type 1 or 2 diabetes, gestational diabetes, chronic hypertension, renal disease, and autoimmune diseases), and multifetal gestation.
What is the recommended treatment for pre eclampsia?
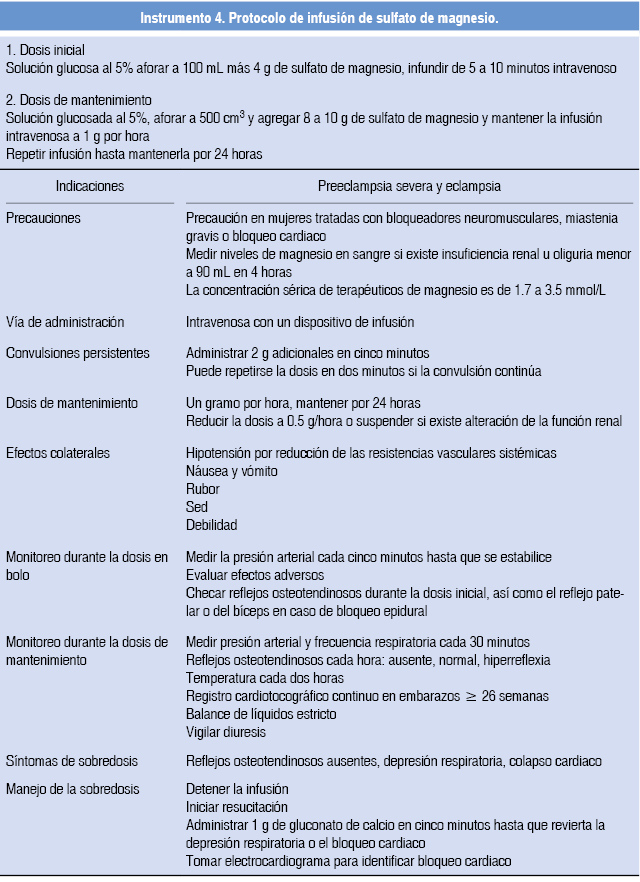
Treatment of severe preeclampsia Antihypertensive drugs to lower blood pressure. Anticonvulsant medication, such as magnesium sulfate, to prevent seizures. Corticosteroids to promote development of your baby's lungs before delivery.
How is preeclampsia treated and prevented?
How can I prevent preeclampsia:Use little or no added salt in your meals.Drink 6-8 glasses of water a day.Avoid fried foods and junk food.Get enough rest.Exercise regularly.Elevate your feet several times during the day.Avoid drinking alcohol.Avoid beverages containing caffeine.More items...
What is the standard treatment for eclampsia?
Eclampsia Treatment Immediate treatment, usually in a hospital, is needed to stop the mother's seizures, treat blood pressure levels that are too high, and deliver the fetus. Magnesium sulfate (a type of mineral) may be given to treat active seizures and prevent future seizures.
Which drug is given to prevent pre eclampsia to become eclampsia?
Because women with preeclampsia can develop seizures (called eclampsia), most women are treated with an anticonvulsant medication during labor and usually for 24 hours after delivery. Intravenous magnesium sulfate is the drug most commonly used to prevent seizures. It is safe for both mother and fetus.
What is the nursing management for a patient with preeclampsia?
The overall management of preeclampsia includes supportive treatment with antihypertensives and anti-epileptics until definitive treatment - delivery. In preeclampsia without severe features, patients are often induced after 37 weeks gestation after with or without corticosteroids to accelerate lung maturity.
What vitamins help prevent preeclampsia?
Folic acid and vitamin B6. May help prevent symptoms in women with a history of preeclampsia and high homocysteine levels. One study found a reduction in preeclampsia with supplementation of a multivitamin with folic acid.
What is difference between preeclampsia and eclampsia?
About Preeclampsia and Eclampsia Preeclampsia and eclampsia are pregnancy-related high blood pressure disorders. Preeclampsia is a sudden spike in blood pressure. Eclampsia is more severe and can include seizures or coma.
Why is MgSO4 given in eclampsia?
Magnesium sulfate therapy is used to prevent seizures in women with preeclampsia. It can also help prolong a pregnancy for up to two days. This allows drugs that speed up your baby's lung development to be administered.
How do you prevent preeclampsia seizures?
The American College of Obstetricians and Gynecologists recommends the use of magnesium sulfate as first-line therapy to prevent seizures in women with preeclampsia.
Which is the drug of choice in eclampsia?
Magnesium sulphate: the drug of choice in eclampsia.
What are the two different steroid drugs for preeclampsia?
During this time, you may receive magnesium sulfate to prevent convulsions. You may also receive other medications to lower your blood pressure, such as hydralazine (Apresoline), and steroids, such as betamethasone to help your baby's lungs develop. You'll also need to stay in the hospital until delivery.
What are the management strategies for preeclampsia?
Management strategies for diagnosed preeclampsia may include close fetal and maternal monitoring, antihypertension medications, and magnesium sulfate. Balance of Benefits and Harms. The USPSTF concludes with moderate certainty that there is a substantial net benefit of screening for preeclampsia in pregnant women.
What is the best way to diagnose hypertension?
The Society of Obstetricians and Gynaecologists of Canada recommends that the diagnosis of hypertension be based on office or in-hospital blood pressure measurements and that all pregnant women should be assessed for proteinuria. It does not recommend screening with biomarkers or Doppler ultrasonography. 30 The National Institute for Health and Care Excellence recommends screening for preeclampsia by obtaining blood pressure measurements and urinalysis for proteinuria at each antenatal visit. 31 The American College of Obstetricians and Gynecologists recommends obtaining blood pressure measurements at every prenatal visit and using a detailed medical history to evaluate for risk factors for preeclampsia. 5, 32
What is the second study?
The second study was a fair-quality, retrospective, before-after comparison cohort study (n=1952) of low-income pregnant Hispanic women. The study did not identify any harms related to preeclampsia diagnosis and birth outcomes when targeted urine protein screening was used for specific indications only compared with routine use in prenatal care. 4, 27
Why is blood pressure important for preeclampsia?
Obtaining blood pressure measurements to screen for preeclampsia could allow for early identification and diagnosis of the condition, resulting in close surveillance and effective treatment to prevent serious complications. The USPSTF has previously established that there is adequate evidence on the accuracy of blood pressure measurements to screen for preeclampsia.
When was the USPSTF recommended screening for preeclampsia?
In 1996 , the USPSTF recommended screening for preeclampsia using office-based blood pressure measurement for all pregnant women at the first prenatal visit and periodically throughout the remainder of the pregnancy (B recommendation). 18 The USPSTF commissioned a systematic evidence review to appraise and update the evidence on screening for preeclampsia.
Is there evidence for screening for preeclampsia?
In addition, there is adequate evidence to bound the harms of screening for and treatment of preeclampsia as no greater than small. Therefore, the USPSTF concludes with moderate certainty that there is a substantial net benefit of screening for preeclampsia in pregnant women.
Is screening for preeclampsia bad?
The USPSTF identified 2 fair-quality studies that reported on potential harms of alternative approaches to screening for preeclampsia. Neither study found evidence of harms, but both were underpowered to provide evidence on rare clinical outcomes. One was a fair-quality trial (n=2764) that found no difference in birth outcomes (eg, low birth weight, preterm birth, or cesarean delivery) when the number of prenatal care visits was reduced from 14 to 9 visits. 4, 23 As noted earlier, this trial was not sufficiently powered to detect differences for rare outcomes related to preeclampsia such as progression to eclampsia, organ failure, stroke, and death.