Mayoclinic.org
Aug 05, 2021 · There is general agreement as to which antihypertensive drugs are appropriate for initial therapy in most patients with hypertension. The major options are: Thiazide-type diuretics Angiotensin-converting enzyme (ACE) inhibitors/angiotensin II receptor blockers (ARBs) Calcium channel blockers
Top10homeremedies.com
Surgical resection is the treatment of choice for pheochromocytoma, because hypertension is cured by tumor resection. In the preoperative phase, …
Medicalnewstoday.com
Treating essential hypertension. The first choice is usually a thiazide diuretic. We concluded in 2004 that the first-choice treatment for hypertension in adults was single-agent therapy with the thiazide diuretic chlortalidone or, when this drug is not available, the thiazide diuretic hydrochlorothiazide.
What is the best treatment for hypertension?
Hence, we believe that beta blockers should not remain first choice in the treatment of primary hypertension and should not be used as reference drugs in future randomised … In comparison with other antihypertensive drugs, the effect of beta …
What is the first-choice treatment for hypertension?
Which of the following is the primary type of drug recommended for patients who have edema or fluid retention with heart failure (HF)? a. Angiotensin receptor antagonist b. Angiotensin converting enzyme inhibitor c. Aldosterone antagonist d. Beta-blocker e. Diuretic
What is the recommended first-line treatment for hypertension?
A patient is prescribed a calcium channel blocker to treat primary hypertension. When teaching the patient about the medication, which of these foods will the healthcare provider advise the patient to avoid? Please choose from one of the following options. Eggs Bananas Oranges Grapefruit Grapefruit
What are the Therapeutic Guidelines for uncomplicated hypertension?
Hypertensive encephalopathy, intracranial hemorrhage, myocardian infarction, flash pulmonary edema, and aortic dissection. What are the treatments of choice for hypertensive emergency? IV antihypertensive medications such as labetalol, nicardipine, nitroprusside and fenoldepam.

What is first line treatment for hypertension?
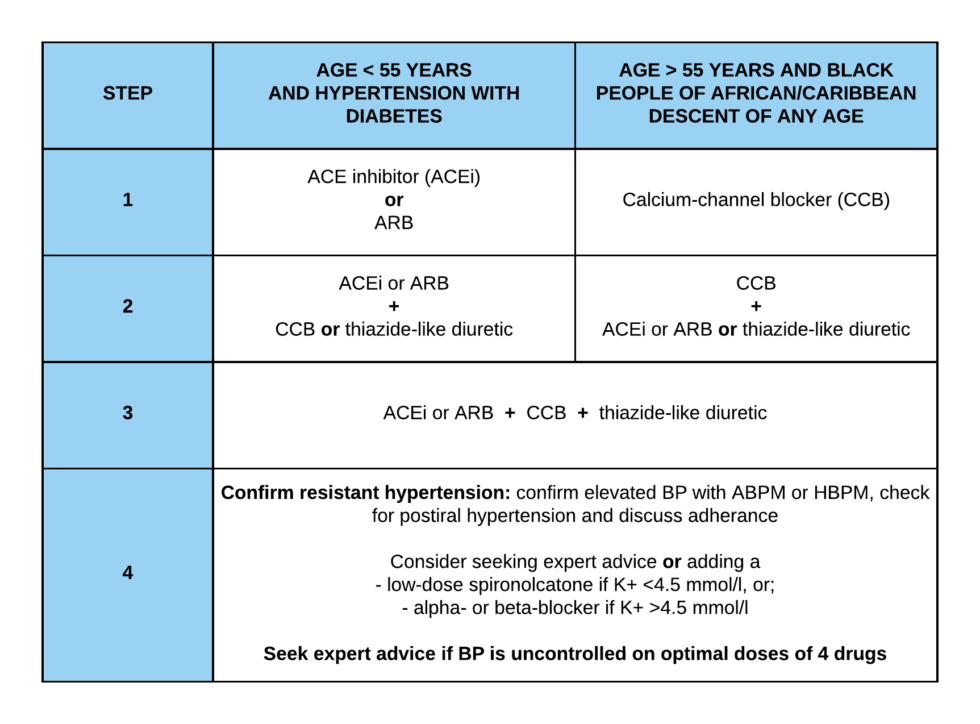
There are three main classes of medication that are usually in the first line of treatment for hypertension: 1. Calcium Channel Blockers (CCB) 2. Angiotensin Converting Enzyme inhibitors (ACE inhibitors or ACE-I) and Angiotensin Receptor Blockers (ARBs) 3. Diuretics.
What is the first drug of choice for hypertension 2020?
Initial first-line therapy for stage 1 hypertension includes thiazide diuretics, CCBs, and ACE inhibitors or ARBs. Two first-line drugs of different classes are recommended with stage 2 hypertension and average BP of 20/10 mm Hg above the BP target.May 7, 2018
What is the best treatment for hypertension?
The two classes of medication are both recommended as "first-line" treatments for high blood pressure: angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs). ACE inhibitors have been around longer and studied more extensively, so doctors prescribe them more often.Jul 26, 2021
What is the most effective treatment for hypertension?
Diuretics are often recommended as the first line of therapy for most people who have high blood pressure. However, your doctor may start a medicine other than a diuretic as the first line of therapy if you have certain medical problems. For example, ACE inhibitors are often a choice for people with diabetes.Sep 20, 2021
What is a revascularization technique for renovascular hypertension?
Aortorenal bypass using a saphenous vein graft or a hypogastric artery is a revascularization technique for renovascular hypertension that has become much less common since the advent of renal artery angioplasty with stenting. Surgical resection is the treatment of choice for pheochromocytoma and for patients with a unilateral solitary aldosterone-producing adenoma, because hypertension is cured by tumor resection. Of note, patients with benign adenomas may be able to be treated with spironolactone instead of surgery. In patients with fibromuscular renal artery disease, angioplasty has a 60-80% success rate for improvement or cure of hypertension. Another intervention that initially seemed to hold great promise for the treatment of resistant hypertension is renal artery denervation. However, more recent controlled studies have suggested little benefit on BP from percutaneous renal denervation therapy, and ongoing studies are testing this intervention using newer techniques. [ 76]
What is the age limit for hypertension?
The American College of Physicians (ACP) and the American Academy of Family Physicians (AAFP) released their guidelines regarding hypertension in adults aged 60 years, including the following [ 72] :
What is the BP goal for kidney transplant?
Adults with hypertension and chronic kidney disease (CKD) should be treated to a BP goal of less than 130/80 mm Hg. After kidney transplantation, it is reasonable to treat patients with hypertension to a BP goal of less than 130/80 mm Hg.
How to lower blood pressure?
Blood pressure may be lowered by 4-9 mm Hg with moderately intense physical activity. [ 5] . These activities include brisk walking for 30 minutes a day, 5 days per week. More intense workouts of 20-30 minutes, 3-4 times a week, may also lower BP and have additional health benefits.
When should beta blockers be used?
Beta-blockers may not be as effective as other first-line agents in patients aged 60 years and older, especially for stroke prevention, and should probably be used when other indications are present, such as heart failure, previous myocardial infarction, and angina. [ 7]
Does magnesium help with BP?
Calcium and magnesium supplementation have elicited small reductions in BP. In population studies, low levels of alcohol consumption have shown a favorable effect on BP, with reductions of 2-4 mm Hg. However, the consumption of 3 or more drinks per day is associated with elevation of BP.
Is chlortalidone an ACE inhibitor?
In one of these trials, chlortalidone was superior to the ACE inhibitor lisinoprilin preventing stroke.
Does thiazide cause hyperglycaemia?
Thiazide diuretics can provoke hyperglycaemia and diabetes, although this does not reduce their efficacy in the prevention of cardiovascular events. As of early 2014, the first-choice treatment for hypertension in nondiabetic adults without cardiovascular or renal disease should be chlortalidone.
What is the goal of uncomplicated hypertension?
Summary. The goal of therapy in uncomplicated hypertension is to reduce cardiovascular risk by lowering the patient's blood pressure. If non-drug treatment is ineffective, the choice of drug treatment is determined by its safety and efficacy. When safety and efficacy are equal the lowest cost drug should be prescribed.
Is thiazide a first line diuretic?
However, for most patients with uncomplicated hypertension low-dose thiazide-type diuretics should be first-line therapy. The choice of add-on therapy, which may be required later in up to two-thirds of patients, is not as clearly defined. Beta blocking drugs and ACE inhibitors are effective when used with a diuretic.
Is it safe to take antihypertensives?
Compared with drugs used for other chronic disorders, antihypertensives are among the safest. They cause very little specific organ toxicity and many of them have been in use for many years so their adverse effects are well known. Periodically there are alarms about particular classes - for example, the precipitation of vascular occlusion with short-acting calcium channel blocking drugs or cardiovascular collapse with hypotension when starting an ACE inhibitor. However, most of these problems can be avoided with appropriate prescribing and monitoring of treatment.
Is thiazide diuretic high risk for diabetes?
Patients with hypertension are often overweight and have an increased likelihood of developing diabetes, independent of treatment. The small extra risk of type 2 diabetes with the long-term use of thiazide diuretics was reported in the 1960s when relatively high doses were used.
Is comparative cost a discriminator?
In the absence of major differences in efficacy, safety and convenience, comparative cost may become the final discriminator . In a Pharmaceutical Benefits Scheme (PBS) which is continually under threat, small differences in cost (to the taxpayer) in treating a condition which affects 10-15% of the population can add up to substantial sums, particularly as treatment is usually lifelong.
Is hypertension a family history?
These patients commonly have a family history of hypertension, but clinical assessment and selective investigation reveal no primary underlying cause of the hypertension.
Treatment
Overview
- Hypertension requiring treatment exists when a patient's blood pressure, measured on at least three separate occasions, exceeds the threshold pressures which predict an increased cardiovascular risk, in the absence of complicating features such as diabetes mellitus and overt cardiovascular disease. These patients commonly have a family history of hypertension, but clin…
Criticism
- Controlled clinical trials are often criticised for their lack of representativeness. This may undermine the doctor's confidence in applying the results to individual patients, however, we have no better evidence than these trials. The differences which occur between trials are often exploited in drug promotion, so how do we account for these discrepancies?
Results
- The differences may reflect the design of the trials. Results from non-randomised studies are more likely to be favourable to the drug of interest than those of randomised trials. Within randomised trials, less weight should be given to the results if allocation to treatment or control arms was not concealed. The populations included in the trials may not be comparable (for exa…
Medical uses
- The criteria by which we select one class of drug as first-line treatment are usually dominated by comparative efficacy. In hypertension all the five major drug classes (low-dose thiazides, beta blockers, calcium channel blockers, angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor antagonists) are efficacious in reducing blood ...
Availability
- While the conclusion of the National Heart Foundation guidelines (2004)5 that 'Drugs from any of the five major classes are suitable for initiation and maintenance of antihypertensive therapy' is correct, this is true only if efficacy is considered alone. Other considerations also have a place in the choice of first-line drugs. The World Health Organization program, the 'Guide to good prescri…
Safety
- Compared with drugs used for other chronic disorders, antihypertensives are among the safest. They cause very little specific organ toxicity and many of them have been in use for many years so their adverse effects are well known. Periodically there are alarms about particular classes - for example, the precipitation of vascular occlusion with short-acting calcium channel blocking drug…
Adverse effects
- Patients with hypertension are often overweight and have an increased likelihood of developing diabetes, independent of treatment. The small extra risk of type 2 diabetes with the long-term use of thiazide diuretics was reported in the 1960s when relatively high doses were used. It is re-emerging as a concern based on recent trials suggesting that a greater proportion of patients ha…
Prevention
- A prudent approach is to measure serum potassium, uric acid and fasting glucose before prescribing and not use diuretics (or beta blockers) if the fasting blood glucose is at, or above, 6.1 mmol/L. Fasting glucose should be monitored periodically in patients on continuing diuretic treatment.
Cost
- In the absence of major differences in efficacy, safety and convenience, comparative cost may become the final discriminator. In a Pharmaceutical Benefits Scheme (PBS) which is continually under threat, small differences in cost (to the taxpayer) in treating a condition which affects 10-15% of the population can add up to substantial sums, particularly as treatment is usually lifelong.
Society and culture
- The comparative cost to the PBS of representative drugs from the five classes of antihypertensive drugs is shown in Table 1. The table includes the dose ranges used in the major studies which showed the efficacy of the drugs in reducing cardiovascular events.
Contraindications
- There will always be the need to tailor treatment to the individual patient, and it will nearly always be inappropriate, for example, to give a patient with gout a diuretic or a patient with asthma a beta blocker. However, for most patients with uncomplicated hypertension low-dose thiazide-type diuretics should be first-line therapy.
Organizations
- Dr Hill was a member of the World Health Organization/International Society of Hypertension group which constructedthe 'Statement on management of hypertension'. ProfessorSmith was Chair of the Writing Group which assembledTherapeutic Guidelines: Cardiovascular, 2003. Neither has anaffiliation with any pharmaceutical company.