Which hypertension medication is best for African American?
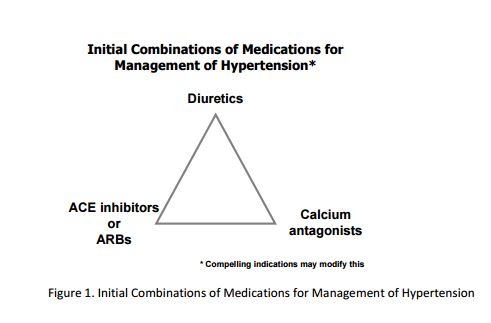
What are the hypertension treatment options for African Americans? Experts recommend Black adults start with either a thiazide diuretic — such as chlorthalidone or hydrochlorothiazide — or a calcium channel blocker like amlodipine (Norvasc).
What is first line treatment for hypertension in African American?
First-line pharmacologic treatment of hypertension for black patients includes thiazide diuretics or calcium channel blockers.
Which is the preferred drug for the treatment of hypertension in African American patients quizlet?
In this cohort, African Americans were most often treated with diuretics, CCBs, and ACE inhibitors. ACE inhibitors appear to be an effective adjunct to diuretic therapy in African Americans due to both the enhanced blood pressure lowering of that combination, and to the decreased production of angiotensin II.
Why are ACE inhibitors not recommended for African black population?
Angiotensin converting enzyme (ACE) inhibitors have been avoided as an initial therapeutic option in the treatment of hypertension in African-Americans. A major reason for this has been the widespread perception of clinicians that these agents have poor blood pressure (BP) lowering efficacy in this population.
How do African Americans treat hypertension?
In the text of the guideline, mentions that diuretics should be the agent of first choice for blacks with hypertension because of their proven effectiveness in clinical trials. For whites, beta-blockers are also an option for first line therapy. Mono-therapy with beta-blockers or ACE-Is is less effective in blacks.
Which antihypertensive medications are the most effective in treating hypertension in African Americans and older adults?
Practice guidelines have long recommended that Black patients with high blood pressure and no comorbidities be treated initially with a thiazide diuretic or a calcium channel blocker (CCB) instead of an angiotensin converting enzyme inhibitor (ACEI) and/or angiotensin receptor blocker (ARB).
Is lisinopril good for African American?
However, lisinopril was associated with an increased risk for heart failure (relative risk [RR] for African Americans=1.32; 95% CI, 1.11–1.58) and stroke (RR for African Americans=1.4; 95% CI, 1.17–1.68), and amlodipine was associated with a higher risk of heart failure (RR in African Americans=1.47; 95% CI, 1.24–1.74) ...
What is a thiazide diuretic drug?
Thiazide diuretics are an FDA-approved class of drugs that inhibit the reabsorption of 3% to 5% of luminal sodium in the distal convoluted tubule of the nephron. By doing so, thiazide diuretics promote natriuresis and diuresis.
What are ACE inhibitors examples?
Angiotensin-converting enzyme inhibitor (ACE inhibitors) drugs include Benazepril (Lotensin), Captopril (Capoten), Enalapril/Enalaprilat (Vasotec oral and injectable), Fosinopril (Monopril), Lisinopril (Zestril and Prinivil), Moexipril (Univasc), Perindopril (Aceon), Quinapril (Accupril), Ramipril (Altace), and ...
Why are calcium channel blockers preferred in African American?
The high efficacy of calcium blockers in patients of African ancestry points to enhanced vascular smooth muscle contractility in this group [11,12,36,37,39,72].
How common is high blood pressure in Black adults?
High blood pressure is much more common in Black people as compared to other groups in the U.S. It affects 56% of Black adults in the U.S. as compared to 48% of white adults, 46% of Asian adults, and 39% of Hispanic adults.
Why is high blood pressure more common and more severe in Black people?
There’s no definitive answer for why high blood pressure is more common and more severe in Black people. Some theories have looked at genetic and environmental factors as possible causes, but it isn’t very well understood.
How is high blood pressure treated?
There are treatment plans that don’t require medication and some that do. The approach to treating high blood pressure depends on how severe it is. A healthy lifestyle can help keep hypertension in check. In fact, it’s recommended you make lifestyle modifications to help lower your blood pressure even if your provider prescribes medication for you.
Non-medication treatments for high blood pressure
For elevated blood pressure (systolic 120 to 129 mmHg and diastolic under 80 mmHg) or stage 1 hypertension (systolic 130 to 139 mmHg or diastolic 80 to 89 mmHg), non-medication management is recommended. This would include diet, exercise, and lifestyle changes.
Medication treatment options for high blood pressure
When high blood pressure persists or has advanced to stage 2 (systolic at least 140 mmHg or diastolic at least 90 mmHg), medication is recommended as additional treatment.
Is high blood pressure treated differently in Black adults?
In general, there are a few types of medications that are considered first-choices treatments for high blood pressure. These include thiazide diuretics (a type of “water pill”), ACE inhibitors, ARBs, and calcium channel blockers. For the most part, these medications are equally effective in lowering blood pressure.
Why are ACE inhibitors and ARBs sometimes not recommended for Black adults?
The simple answer is that these medications tend to not work as well in Black people. The reason for this boils down to the way ACE inhibitors and ARBs work.
What is the best treatment for African Americans with hypertension?
In African Americans with hypertension, therapy is best initiated with the low-sodium Dietary Approaches to Stop Hypertension (DASH) diet and a thiazide-type diuretic (strength of recommendation [SOR]: A, based on randomized controlled trials).
What is the blood pressure of African Americans?
Three large cohort studies determined that African Americans have a higher prevalence of hypertension and worse cardiovascular and renal outcomes when compared with white Americans. For African American patients, the standard blood pressure goals apply: below 140/90 mm Hg with uncomplicated hypertension and below 130/80 with diabetes or renal disease. 1
What is the best treatment for black people with hypertension?
The American College of Cardiology and American Heart Association 2017 hypertension guidelines suggest initial therapy of a calcium channel blocker (CCB) or thiazide diuretic for black patients. Further, it states that two drugs are often needed for treatment of hypertension in black patients.
What is the best medication for black patients?
The American Society of Hypertension and the International Society of Hypertension recommends a CCB or thiazide diuretic (CCB preferred, but thiazide diuretic if cost is a concern) as initial drugs of choice for black patients. If additional treatment is indicated, they suggest adding an ACE-I or ARB.
Do black people have hypertension?
Background: Black patients have a higher prevalence of hypertension, treatment resistant hypertension, and poorer blood pressure control. It is known that certain antihypertensive agents work better and have different adverse drug event frequencies in black patient populations, which guides monotherapy. However, various guidelines provide different ...
Is CCB a second agent?
Joint National Committee 8 recommends initial therapies of a thiazide diuretic or CCB in black patients, but does not provide specific guidance on the best second agent to choose. In general, it recommends adding a CCB, thiazide diuretic, ACE-I, or ARB as a second drug if a patient is not responding to monotherapy.
What is the best medicine for high blood pressure in African Americans?
Recommended Medications for High Blood Pressure in African-Americans. Calcium Channel Blockers (CCB’s) Calcium Channel Blockers (CCB’s) are recommended for first line use for African Americans by JNC 8. They should be used in combination with Thiazide Diuretics. Some are listed below by generic name: Nifedipine.
What is ACE inhibitor?
ACE Inhibitors are used with Calcium Channel Blockers and Thiazide Diuretics for chronic kidney disease and high blood pressure in African Americans.
When was the first document to focus primarily on HTN in blacks or in any black population?
Accordingly, in March of 2003, the ISHIB published a consensus statement on the “Management of High Blood Pressure in African American,” 1 the first such document to focus primarily on HTN in blacks or in any black population.
What are the beliefs of black people with HTN?
Nonbiomedical beliefs appear to be relatively common among blacks with HTN. A study of 93 blacks with HTN subjected to open-ended interviews during routine ambulatory clinic visits found that 38% believed that HTN could be cured, 38% believed that taking antihypertensive medication lifelong was not necessary, and 23% thought that antihypertensive medications needed to be taken only when experiencing symptoms. 64 Clearly, these beliefs could negatively influence the likelihood that blacks with HTN will seek treatment and, once prescribed, adherence to treatment over the long term.
What is the recommended BP level for hypertensive patients?
For hypertensive patients with evidence of target-organ damage, preclinical CVD, or a history of CVD, we recommend maintaining BP levels consistently below the target level of 130/80 mm Hg (see Table 1 ). Patients in this category almost always have multiple risk factors and, because of their known CVD, have much higher absolute CVD risk at a given level of BP than do individuals with similar BP levels but without evidence of pressure-related target-organ injury, preclinical CVD, or overt CVD. Patients in this secondary prevention group will manifest proteinuria (albuminuria; spot urine albumin:creatinine ratio >200 mg/g), depressed renal function (estimated glomerular filtration rate [eGFR] <60 mL/min per 1.73 m 2 ), electrocardiographic (or echocardiographic) evidence of LVH, metabolic syndrome, a Framingham risk score corresponding to >20% 10-year CHD risk, the presence of “prediabetes” (glucose intolerance [2-hour postload glucose ≥140 mg/dL] or impaired fasting glucose [100 to 125 mg/dL]), diabetes mellitus, and/or overt clinical CVD; this risk category includes all patients considered by JNC 7 to be high-risk hypertensives. Virtually all of the above manifestations of target-organ injury and preclinical CVD have been linked to resistance to antihypertensive treatment or to slower attainment of goal BP. The majority of patients in this risk stratum will require multiple antihypertensive drugs to consistently maintain BP levels below the target level of 130/80 mm Hg.
What is the prevalence of OSA in hypertensive populations?
The prevalence of OSA in hypertensive populations is estimated to range between 30% and 40%. 76,118 OSA is more common in blacks than whites, at least at the extremes of age (<25 years and ≥65 years). 119–121 The severity of sleep apnea has been determined by the apnea (complete cessation of airflow for 10 seconds)-hypopnea (reduction in airflow followed by arousal from sleep or a drop in oxyhemoglobin saturation) index. 122 The severity of OSA directly relates to greater body weight, a higher body mass index, and a larger neck circumference. Weight gain (10% of body weight) has been linked to significant increases in apnea-hypopnea index and an even more striking risk for developing moderate-to-severe OSA, 123 whereas weight loss improves the apnea-hypopnea index. 124 OSA has been recognized as a risk factor for HTN, 125 a nondipping nocturnal BP pattern, and increased BP variability. 76 Masked HTN (normal office BP but elevated ambulatory BP) was found in 30.0% of individuals with sleep apnea, a prevalence almost identical to that of sustained HTN (35.4%). 126 Although CVD risk falls with continuous positive airway pressure, few data show sustained reductions in BP after such therapy.
What is resistant HTN?
Resistant HTN has been defined as the lack of BP control on ≥3 adequately dosed drugs of different classes (including a diuretic) or controlled BP on ≥4 agents inclusive of a diuretic. The rising numbers of Americans with HTN and subsequent resistant HTN have been attributed to the rapidly increasing prevalence of comorbidities, such as obesity, type 2 diabetes mellitus, and CKD. 158–160 Treatable causes of resistant HTN should be sought and addressed or eliminated to the greatest degree feasible. These include OSA and use of modalities that raise BP (high-salt/low-potassium diet, excessive alcohol intake, nonsteroidal antiinflammatory agents, decongestants, cocaine, etc). Table 6 displays recommendations for attaining BP control in patients with resistant HTN including the use of a diuretic that is appropriate to the level of kidney function. Impedance cardiography appears to be a useful therapeutic decision aid. Three-month HTN control rates in HTN specialist 161 and primary care 162 have been higher when drug selections have been guided by hemodynamic abnormalities.
Is salt sensitivity more common in blacks than whites?
Salt sensitivity is more common in black than white hypertensives and is also present, albeit to a lesser degree, in normotensive blacks. 104 Nevertheless, >50% of both blacks and whites with HTN will manifest salt sensitivity. 105 Salt sensitivity is a reversible intermediate BP phenotype that has been linked to obesity in both blacks and whites 106,107 and is a likely physiological contributor to salt and water retention and plasma volume expansion that occurs during antihypertensive drug therapy. Administration of dietary sodium chloride in potassium-deficient blacks causes renal vasoconstriction that directly correlates to the rise in BP; however, both the renal vasoconstriction and the rise in BP can be abolished by high-dose (170 mmol/d) potassium bicarbonate. 108 Interestingly, there is a suggestion of augmented BP lowering to calcium channel blockers (CCB) in black salt-sensitive hypertensives when dietary sodium intake is high. 109 Conversely, drugs acting primarily on the RAS produced a lesser BP response if the patient was salt sensitive and ingesting a high-salt diet. 110
Should lifestyle modifications be initiated in all patients with HTN?
Lifestyle modifications should be initiated in all patients with HTN, whether pharmacotherapy is planned . BP can be brought to goal in the majority of patients if antihypertensive medications are correctly dosed or combined. As BP is brought to goal, attention should be specifically directed to long-term adherence to therapy.