Is oxcarbazepine better than carbamazepine for trigeminal neuralgia?
A review study discussing the pharmacological options to treat trigeminal neuralgia concluded that carbamazepine & oxcarbazepine are the first choice of drugs(1). Oxcarbazepine showed equal efficacy in reducing pain attacks with better tolerability & less side effects (1) .Aug 9, 2021
Which is better Trileptal or Tegretol?
Tegretol (carbamazepine) is useful for preventing seizures and relieving certain types of nerve pain, but reduces how well many other medications work. Trileptal (Oxcarbazepine) is effective at lowering the frequency of seizures, especially for people with partial seizures.
Is oxcarbazepine better than carbamazepine?
OXC is often better tolerated than CBZ and causes fewer rashes than CBZ. Add-on or substitution treatment with OXC was effective in controlled trials even when CBZ did not achieve sufficient seizure control. This constitutes compelling clinical evidence that OXC and CBZ are distinctly different medications.
Can trileptal treat trigeminal neuralgia?
Trileptal, or oxycarbemazepine, is a form of Tegretol® that is becoming more widely prescribed for a variety of conditions. It has recently been found to be effective for some patients with trigeminal neuralgia.
Is Trileptal similar to Tegretol?
Are Tegretol and Trileptal the Same Thing? Tegretol (carbamazepine) and Trileptal (oxcarbazepine) are anticonvulsants used to treat seizures. Tegretol is also used to treat nerve pain such as trigeminal neuralgia and diabetic neuropathy, and to treat bipolar disorder.
What's the difference between Oxcarbazepine and Tegretol?
Oxcarbazepine is a structural analog of carbamazepine that follows a different metabolic pathway, resulting in several clinical advantages. Unlike carbamazepine, which is converted to an epoxide metabolite, oxcarbazepine is rapidly converted to its monohydroxy derivative (MHD), which is the main active metabolite.
What is an alternative to carbamazepine?
The findings support NICE recommendations to use carbamazepine or lamotrigine as first-line therapies for epilepsy with partial seizures, with levetiracetam as an alternative. Sodium valproate or lamotrigine are recommended for people with generalised tonic-clonic seizures, and levetiracetam is an alternative option.Sep 12, 2017
Is Tegretol and carbamazepine the same thing?
Tegretol, generic name carbamazepine, is an anticonvulsant that is sometimes prescribed as a mood stabilizer in bipolar disorder. In addition to seizures and bipolar disorder, it's also prescribed for pain relief in trigeminal neuralgia.Mar 1, 2020
What are the long term side effects of Trileptal?
Tell your doctor right away if you have any serious side effects, including: double vision, change in vision, involuntary eye movements, difficulty speaking, difficulty concentrating, loss of coordination, trouble walking (abnormal gait), uncontrolled muscle movements (tremor), dulled sense of touch, easy bleeding/ ...
Does Tegretol cure trigeminal neuralgia?
To treat trigeminal neuralgia, your doctor usually will prescribe medications to lessen or block the pain signals sent to your brain. Anticonvulsants. Doctors usually prescribe carbamazepine (Tegretol, Carbatrol, others) for trigeminal neuralgia, and it's been shown to be effective in treating the condition.Jan 26, 2022
How long do you have to take Tegretol for trigeminal neuralgia?
Patients usually begin to respond to the treatment within four to 12 weeks post-treatment, but some patients require as much as six to 12 months for the full response. Most patients remain on full doses of their trigeminal neuralgia medication for at least three to six months after treatment.
What is the most effective treatment for trigeminal neuralgia?
Microvascular decompression (MVD) surgery is regarded as the most long-lasting treatment for trigeminal neuralgia caused by blood vessel compression, and it helps about 80% of people with this diagnosis.
What is the treatment for trigeminal neuralgia?
Introduction Today, trigeminal neuralgia is usually treated with drugs called anti-convulsants, which include carbamazepine (Tegretol®), phenytoin (Dilantin®), oxycarbazepine (Trileptal®), and gabapentin (Neurontin®). Phenytoin was first introduced in 1942, and in 1962 carbamazepine became the most commonly used drug.
How much Tegretol should I take a day?
Like Tegretol®, it is an anti-seizure drug, but the side effects are less severe and less frequently experienced. The dose usually begins at 300 mg twice a day and is gradually increased to achieve pain control. The maximum dose is 2400-3000 mg per day. Common side effects are nausea, vomiting, dizziness, fatigue and tremors.
How long does it take for carbamazepine to decrease?
If side effects are severe, the daily dose of carbamazepine may be decreased for 1 to 3 days, before trying to increase the daily dose again. There are also rare but serious reactions to carbamazepine that are not dose related. These include an allergic skin rash that may form any time after the medication is started.
What are the side effects of nystagmus?
These dose-dependant side effects include nystagmus (rapid movements of the eye), ataxia (decreased coordination), dysarthria (speech difficulty), ophthalmoplegia (paralysis of eye movements) as well as drowsiness and mental confusion. Other effects of the medication may include gingival hyperplasia (enlargement of the gums in the mouth) ...
What happens if you take carbamazepine?
Two to six percent of sufferers who take carbamazepine develop blood disorders including leukopenia or agranulocytosis (drop in the number of white blood cells), or aplastic anemia (when the bone marrow stops producing blood cells) . Other rare complications include liver toxicity, water intoxication (retention of water), ...
What is the best treatment for TN?
Treatment is usually initiated with one drug, such as Tegretol® or Neurontin®. The dose is increased as needed and tolerated.
Is gabapentin a neurotransmitter?
Gabapentin is an anti-epileptic drug that is structurally related to the neurotransmitter GABA. This drug is almost as effective as carbamazepine but involves fewer side effects . The starting dose is usually 300mg three times a day and this is increased to a maximal dose. The most common adverse reactions include somnolence (sleepiness), ataxia (decreased coordination), fatigue, and nystagmus (rapid movements of the eye). There is no known interaction with Tegretol® or Dilantin®, permitting usage of these drugs in combination with Neurontin®. As with all of these drugs, rapid discontinuation should be avoided as severe withdrawal reactions may occur.
What medications treat trigeminal neuralgia?
Typical meds: Tegretol, neurontin, Lyrica ( pregabalin) are standard first line treatment medications.
What is the best procudure for trigeminal neuralgia ?
COMPLEX: There are several surgical approaches, but success may be dependent on whether there is vascular or bony compression of the trigeminal nerve at the base of the brain. This is a relatively safe procedure these days. Medical treatment may work, and many choices exist.
What is the rating of Oxcarbazepine?
Also known as: Trileptal, Oxtellar XR. Oxcarbazepine has an average rating of 8.1 out of 10 from a total of 48 ratings for the treatment of Trigeminal Neuralgia. 77% of users who reviewed this medication reported a positive effect, while 13% reported a negative effect. Filter by condition.
Does Oxcarbazepine help with nausea?
As far as drugs go I feel oxcarbazepine has helped the most. It took some time for my body to get over the nausea but eventually became used to it. Just take nausea medication to help while your body gets used to it. The fatigue, dizziness, and lack of thought process is improving as I've slowly reduce the meds.”.
Does carbamazepine cause brain fog?
First tried carbamazepine which took away the pain by caused brain fog and increased weakness. Oxcarbazepine at 75 mg (slow release) a day took away pain with no side effects. Just two weeks in it's effectiveness is diminishing. Now get pain while eating, touching face etc.
What is the drug used for seizures?
Tegretol ( carbamazepine) and Trileptal ( oxcarbazepine) are anticonvulsants used to treat seizures. Tegretol is also used to treat nerve pain such as trigeminal neuralgia and diabetic neuropathy, and to treat bipolar disorder.
What is trileptal used for?
What is Trileptal? Trileptal (oxcarbazepine) is an anticonvulsant, or antiepileptic drug, used to treat partial seizures in adults and children who are at least 2 years old. Trileptal is available in generic form.
How much XR is needed for trigeminal neuralgia?
The starting dose to treat trigeminal neuralgia is 100 mg twice daily for tablets or XR tablets, or ½ tsp 4 times daily for suspension, for a total daily dose of 200 mg. Control of pain is maintained in most patients with 400-800 mg daily. Consult your doctor for pediatric doses.
What are the side effects of trileptal?
Tell your doctor if you have serious side effects of Trileptal including: changes in vision, involuntary eye movements, difficulty speaking, difficulty concentrating, loss of coordination,
Is there a missing drug warning?
Any missing drug warnings or information does not in any way guarantee the safety, effectiveness, or the lack of adverse effects of any drug. The drug information provided is intended for reference only and should not be used as a substitute for medical advice.
Does RXList.com update drug information?
As drug information can and will change at any time, RxList.com makes every effort to update its drug information. Due to the time-sensitive nature of drug information, RxList.com makes no guarantees that the information provided is the most current.
How long does it take for oxcarbazepine to be metabolized?
Oxcarbazepine is administered orally. Following absorption, it undergoes rapid reduction in the liver to MHD. Peak MHD plasma levels are reached in 4—6 hours while steady state levels are attained within 2—3 days of twice daily dosing. The half-lives of oxcarbazepine and MHD are 2 and 9 hours, respectively. MHD is metabolized primarily through conjugation to minor metabolites. About 4% of MHD is oxidized through hepatic CYP3A4/5 isoenzymes. More than 95% of the dose is renally excreted; however, less than 1% is unchanged oxcarbazepine. Almost one-half of a dose is eliminated as metabolites of MHD. Less than 4% of a dose is excreted in the feces.
How long should Oxcarbazepine be titrated?
Oxcarbazepine should be titrated upward by 600 mg/day every week over 2 to 4 weeks to achieve the recommended dose of 2,400 mg/day. The dosage (s) of concurrent anticonvulsants should be completely withdrawn over 3 to 6 weeks as tolerated.
Is dasabuvir a contraindicated drug?
Dasabuvir; Ombitasvir; Paritaprevir; Ritonavir: (Contraindicated) Concurrent administration of oxcarbazepine with dasabuvir; ombitasvir; paritaprevir; ritonavir is contraindicated. Taking these drugs together could result in decreased plasma concentrations of paritaprevir, ritonavir, and dasabuvir, which may affect antiviral efficacy. Oxcarbazepine is a moderate inducer of the hepatic isoenzyme CYP3A4, and ritonavir, paritaprevir, and dasabuvir (minor) are CYP3A4 substrates. (Major) Concurrent administration of oxcarbazepine with ritonavir should be undertaken with caution and careful monitoring of antiviral efficacy. Oxcarbazepine is a moderate inducer of the hepatic isoenzyme CYP3A4, and ritonavir is a CYP3A4 substrate.
Is carbinoxamine a moderate drug?
Carbinoxamine; Hydrocodone; Pseudoephedrine: (Moderate) Monitor for reduced efficacy of hydrocodone and signs of opioid withdrawal if coadministration with oxcarbazepine is necessary; consider increasing the dose of hydrocodone as needed.
Does carbamazepine decrease MHD?
Coadministration of carbamazepine (400 to 2,000 mg/day) with oxcarbazepine (900 mg/day) decreased MHD concentrations by 40% . Strong CYP3A4 inducers or UGT inducers have been shown to decrease plasma concentrations of MHD. Carbamazepine is a strong CYP3A4 inducer and a UGT inducer.
Is cabotegravir contraindicated?
Cabotegravir: (Contraindicated) Coadministration of cabotegravir and oxcarbazepine is contraindicated due to the potential for significant decreases in the plasma concentrations of cabotegravir, which may result in potential loss of virologic response and development of resistance. Cabotegravir is a substrate for UGT1A1 and UGT1A9; oxcarbazepine is an inducer of UGT. Coadministration with another UGT inducer decreased cabotegravir exposure by 59%.
Does aspirin affect dihydrocodeine?
Aspirin, ASA; Caffeine; Dihydrocodeine: (Moderate) Concomitant use of dihydrocodeine with oxcarbazepine can decrease dihydrocodeine levels , resulting in less metabolism by CYP2D6 and decreased dihydromorphine concentrations; this may result in decreased efficacy or onset of a withdrawal syndrome in patients who have developed physical dependence. If coadministration is necessary, monitor for reduced efficacy of dihydrocodeine and signs of opioid withdrawal; consider increasing the dose of dihydrocodeine as needed. If oxcarbazepine is discontinued, consider a dose reduction of dihydrocodeine and frequently monitor for signs or respiratory depression and sedation. Oxcarbazepine is a weak inducer of CYP3A4, an isoenzyme partially responsible for the metabolism of dihydrocodeine.
What is the best treatment for trigeminal neuralgia?
Although carbamazepine and oxcarbazepine are the first-line treatment, other drugs may be useful for pain control in trigeminal neuralgia. Among them, the anticonvulsants gabapentin, pregabalin, lamotrigine and phenytoin, baclofen, and botulinum toxin type A can be coadministered with carbamazepine or oxcarbazepine for a synergistic approach.
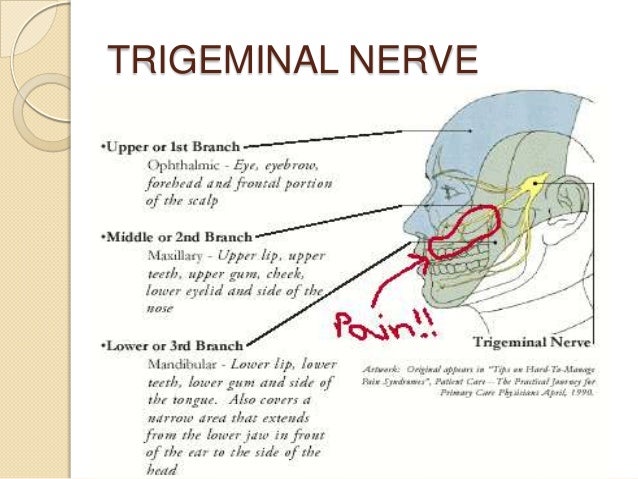
What is the trigeminal nerve?
The trigeminal nerve (V) is the fifth and largest of all cranial nerves, and it is responsible for detecting sensory stimuli that arise from the craniofacial area. The nerve is divided into three branches: ophthalmic (V1), maxillary (V2), ...
What are the three branches of the trigeminal nerve?
The nerve is divided into three branches: ophthalmic (V1) , maxillary (V2), and mandibular (V3); their cell bodies are located in the tri …. The trigeminal nerve (V) is the fifth and largest of all cranial nerves, and it is responsible for detecting sensory stimuli that arise from the craniofacial area. The nerve is divided into three branches: ...
What is the etiology of triceminal neuralgia?
Trigeminal neuralgia is characterized by sudden, brief, and excruciating facial pain attacks in one or more of the V branches, leading to a severe reduction in the quality of life of affected patients. Trigeminal neuralgia etiology can be classified into idiopathic, classic, and secondary.
Which cranial nerve is responsible for detecting sensory stimuli?
The trigeminal nerve (V) is the fifth and largest of all cranial nerves, and it is responsible for detecting sensory stimuli that arise from the craniofacial area. The nerve is divided into three branches: ophthalmic (V1), maxillary (V2), and mandibular (V3); their cell bodies are located in the trigeminal ganglia and they make connections ...
Which part of the brain is responsible for interpreting sensory information?
Ascending projections via the trigeminothalamic tract transmit information to the thalamus and other brain regions responsible for interpreting sensory information. One of the most common forms of craniofacial pain is trigeminal neuralgia.