
What are the goals for treatment of hypernatremia?
May 13, 2014 · In addition, these patients may exacerbate their hyponatremia through the ingestion of solute-poor fluids (e.g., water or tea). 9 The most common treatment option proposed for patients with hypovolemic hyponatremia is replacement of both salt and water through the intravenous infusion of sodium chloride solutions. 9 – 11 Our review did not …
How quickly can acute symptomatic hyponatremia be corrected?
6 rows · Apr 06, 2018 · Lowering plasma sodium below 120 mEq/L within hours causes severe cerebral edema ( 7 – 9 ). Rapid ...
When to treat hyponatremia?
Feb 07, 2017 · Diagnosis and Treatment of Hyponatremia: Compilation of the Guidelines Abstract. Hyponatremia is a common water balance disorder that often poses a diagnostic or therapeutic challenge. Vasopressin. Arginine vasopressin (the antidiuretic hormone) plays a central role in the pathogenesis of ...
What are the treatment guidelines for hyponatremia?
May 15, 2004 · In patients with chronic hyponatremia, fluid restriction is the mainstay of treatment, with demeclocycline therapy reserved for use in persistent cases.

How to treat hyponatremia?
If you have severe, acute hyponatremia, you'll need more-aggressive treatment. Options include: 1 Intravenous fluids. Your doctor may recommend IV sodium solution to slowly raise the sodium levels in your blood. This requires a stay in the hospital for frequent monitoring of sodium levels as too rapid of a correction is dangerous. 2 Medications. You may take medications to manage the signs and symptoms of hyponatremia, such as headaches, nausea and seizures.
What to write down when taking a medication?
Write down key medical information, including other medical problems for which you are being treated and the names of all medications, vitamins, supplements or other natural remedies you are taking.
What to do if you have a headache and nausea?
Preparing for your appointment. Seek emergency care for anyone who develops severe signs and symptoms of hyponatremia, such as nausea and vomiting, confusion, seizures, or lost consciousness. Call your doctor if you know you are at risk of hyponatremia and are experiencing nausea, headaches, cramping or weakness.
Can you take medication for hyponatremia?
Medications. You may take medications to manage the signs and symptoms of hyponatremia, such as headaches, nausea and seizures.
Can you cut back on fluids with hyponatremia?
Hyponatremia treatment is aimed at addressing the underlying cause, if possible. If you have moderate, chronic hyponatremia due to your diet, diuretics or drinking too much water, your doctor may recommend temporarily cutting back on fluids.
Can a doctor diagnose hyponatremia?
However, because the signs and symptoms of hyponatremia occur in many conditions, it's impossible to diagnose the condition based on a physical exam alone.
What causes brain damage in experimental hyponatremia?
Fatal brain damage in untreated acute experimental hyponatremia is caused by cerebral edema; demyelinating brain lesions in chronic hyponatremia are complications of excessively rapid correction. Challenges in Translating Experimental Observations to the Bedside.
How long does it take for Na to increase?
Increase in Na in 48 h, mEq/L
Does hyponatremia cause seizures?
In symptomatic chronic hyponatremia, the possibility of an acute exacerbation raises concerns for seizures or even herniation. Conversely, despite a history of severe polydipsia, the possibility of underlying chronic hyponatremia raises concern for osmotic demyelination if correction is excessive.
Is hyponatremia chronic or acute?
The designations “acute” and “chronic” hyponatremia do not always work well in practice. Many physicians are confused by the terms, believing “chronic” to mean hyponatremia that has been present for months and “acute” to mean hyponatremia that has recently become symptomatic. Even when currently accepted time-based definitions (>48 hours = chronic; <48 hours = acute) are understood, the true duration of hyponatremia is seldom known. In symptomatic chronic hyponatremia, the possibility of an acute exacerbation raises concerns for seizures or even herniation. Conversely, despite a history of severe polydipsia, the possibility of underlying chronic hyponatremia raises concern for osmotic demyelination if correction is excessive.
Can hyponatremia cause death?
Patients with severe (serum sodium ≤120 mEq/L), symptomatic hyponatremia can develop life-threatening or fatal complications from cerebral edema if treatment is inadequate and permanent neurologic disability from osmotic demyelination if treatment is excessive. Unfortunately, as is true of all electrolyte disturbances, there are no randomized trials to guide the treatment of this challenging disorder. Rather, therapeutic decisions rest on physiologic principles, animal models, observational studies, and single-patient reports. European guidelines and recommendations of an American Expert panel have come to similar conclusions on how much correction of hyponatremia is enough and how much is too much, but there are important differences. We review the evidence supporting these recommendations, identifying areas that rest on relatively solid ground and highlighting areas in greatest need of additional data.
Does hyponatremia resolve spontaneously?
Correction rates are affected by the underlying cause (30,31). Hyponatremia due to heart failure, cirrhosis, kidney injury, or malignancy does not spontaneously resolve and may not be treated; patients with these disorders often die in the hospital. By contrast, hyponatremia caused by diuretics or antidepressants resolves after medications are discontinued; patients with medication-induced hyponatremia rarely die in the hospital.
Does hyponatremia increase mortality?
Some authors have correlated correction rates of hyponatremia to mortality, concluding that inadequate treatment increases the risk of dying (24–27). However, mortality can be a very misleading outcome measure.
How to treat hyponatremia?
Except for hypovolemic hyponatremia, the treatment of chronic hyponatremia relies on reducing free water intake and/or increasing renal free water excretion (Table 2). Fluid restriction (<1 L/d) is often the cornerstone of the therapy for chronic hyponatremia.24The urine to serum electrolyte ratio ([UNa+ urine potassium concentration]/SNa) indicates if the patient is in an antidiuretic or aquaretic phase, and can also help estimate the degree of fluid restriction required to increase SNa.3,11,24,82For patients with a ratio>1 (indicating concentrated urine), <500 ml fluid/d is recommended, which is difficult to adhere to. Winzeler et al.recently showed that in patients with SIAD fluid restriction is effective in 59% of patients.83Predictors of nonresponse were a UNa≥130 mmol/L and UOsm≥500 mOsm/kg.83This implies that in patients with chronic hyponatremia pharmacologic therapy is often required to increase renal free water excretion. This can be achieved by treatment with loop diuretics, urea, vasopressin receptor antagonists (“vaptans”), or demeclocycline. The two guidelines diverge in their recommendations regarding pharmacologic therapy for SIAD and hypervolemic hyponatremia (Table 2). This was the case especially for vaptans, which will therefore be discussed in more detail below.
What is the SNa of hyponatremia?
Hyponatremia (serum sodium [SNa] <136 mmol/L) is a common water balance disorder that often poses a diagnostic or therapeutic challenge .1This may explain why management of hyponatremia is still suboptimal, as also recently illustrated by a hyponatremia registry.2Hyponatremia is not a disease but rather a pathophysiologic process indicating disturbed water homeostasis.3Therefore, hyponatremia should be further classified in order to provide directions for diagnosis and treatment (Table 1). These classifications illustrate that hyponatremia is a very heterogeneous disorder. This has complicated clinical studies, because “the” patient with hyponatremia does not exist. Instead, the underlying disease that is complicated by hyponatremia usually characterizes patients with hyponatremia.4,5The most common causes of hyponatremia are the syndrome of inappropriate antidiuresis (SIAD), diuretic use, polydipsia, adrenal insufficiency, hypovolemia, heart failure, and liver cirrhosis (the latter two are often collectively referred to as “hypervolemic hyponatremia”). Although recent years have seen several developments in the diagnosis and treatment of hyponatremia, the evidence base is still limited. To capture the current approach to hyponatremia, two sets of guidelines have been developed, one by professional organizations from within the United States (“United States guideline”) and one from within Europe (“European guideline,” in which the authors of this review participated).6–9The professional organizations involved in the United States guideline were Tufts University Office of Continuing Education and In 2 MedEd; the initiative was also supported by an unrestricted educational grant from Otsuka America Pharmaceutical.9The professional organizations involved in the European guideline were the European Renal Association–European Dialysis and Transplantation Association, the European Society of Endocrinology, and the European Society of Intensive Care Medicine.6–8The United States guideline refrained from using a quality-of-evidence scoring system due to the limited evidence. Instead, the guideline was on the basis of expert panel recommendations, which relied on a critical evaluation of relevant literature by the panel members. The European guideline did perform systematic reviews of the available evidence using the Grading of Recommendations Assessment Development and Evaluation scoring system. Both guideline committees were interdisciplinary, and the European guideline was endorsed by the European societies of nephrology, endocrinology, and intensive care.6–8This brief review will compare the two guidelines to discuss the diagnosis and treatment of hyponatremia, while also highlighting recent developments. Because of the breadth of both guidelines, this review will focus on the salient features. To place both guidelines in perspective we will integrate in our discussion the pertinent comments published after their release.10–13
What is the role of arginine vasopressin in hyponatremia?
Arginine vasopressin (the antidiuretic hormone) plays a central role in the pathogenesis of hyponatremia. In one study, nonosmotic secretion of vasopressin was detected in 97% of patients with hyponatremia.35Because hypotonicity normally suppresses vasopressin, the reasons for nonosmotic vasopressin release should be considered.36“Appropriate” vasopressin release is due to hypovolemia or low effective arterial blood volume, both of which activate baroreceptors to cause vasopressin release. Although one might expect thiazide-induced hyponatremia to be due to hypovolemia secondary to saliuresis, this is not the case.37Instead, the pathogenesis appears to be a combination of polydipsia and impaired urea-mediated water excretion.37,38“Inappropriate” vasopressin release is usually caused by the effect of an underlying disease or drugs on central osmoreceptors; alternatively, vasopressin can be produced ectopically (e.g., in small cell lung cancer or olfactory neuroblastoma).3,39,40In addition, hypocortisolism increases vasopressin release, because corticotropin-releasing hormone normally suppresses vasopressin.41Although rare, secondary and even primary adrenal insufficiency may mimic SIAD and can be missed without appropriate testing.42–44Although the kidney usually limits the degree of hyponatremia in SIAD (“vasopressin escape”45), it can also cause antidiuresis independent of vasopressin.46,47A specific example is gain-of-function mutations of the vasopressin type 2 receptor causing hereditary hyponatremia (“nephrogenic SIAD”).48Despite the pathogenetic role of vasopressin in hyponatremia, plasma vasopressin is rarely measured in clinical practice. This has two reasons. First, UOsmaccurately reflects vasopressin activity, and, therefore, this more readily available parameter can be used instead. Second, vasopressin is difficult to measure reliably in nonexpert laboratories, because it binds to platelets, it is unstable in isolated plasma, and commercial assays are not very sensitive for low concentrations.49These limitations, however, have largely been resolved by the development of an assay for copeptin.50
When to not recommend SNa?
a“Do not recommend” when SNa<130 mmol/L, “ recommend against” when SNa<125 mmol/L.
Does hyponatremia correlate with symptoms?
Symptoms do not always correlate with degree of hyponatremia
What is the treatment for hyponatremia?
In other cases of hyponatremia, you may need intravenous electrolyte solutions and medications.
Why do older people have hyponatremia?
Older adults may have more contributing factors for hyponatremia, including age-related changes, taking certain medications and a greater likelihood of developing a chronic disease that alters the body's sodium balance.
What happens when the sodium in your blood is abnormally low?
Hyponatremia occurs when the concentration of sodium in your blood is abnormally low. Sodium is an electrolyte, and it helps regulate the amount of water that's in and around your cells.
What is the normal sodium level?
A normal blood sodium level is between 135 and 145 milliequivalents per liter (mEq/L). Hyponatremia occurs when the sodium in your blood falls below 135 mEq/L. Many possible conditions and lifestyle factors can lead to hyponatremia, including: Certain medications. Some medications, such as some water pills (diuretics), ...
How to prevent low sodium?
Getting treatment for conditions that contribute to hyponatremia, such as adrenal gland insufficiency, can help prevent low blood sodium. Educate yourself. If you have a medical condition that increases your risk of hyponatremia or you take diuretic medications, be aware of the signs and symptoms of low blood sodium.
Why does my body lose sodium?
Chronic, severe vomiting or diarrhea and other causes of dehydration. This causes your body to lose electrolytes, such as sodium, and also increases ADH levels. Drinking too much water. Drinking excessive amounts of water can cause low sodium by overwhelming the kidneys' ability to excrete water.
What causes sodium to be low?
Heart, kidney and liver problems. Congestive heart failure and certain diseases affecting the kidneys or liver can cause fluids to accumulate in your body, which dilutes the sodium in your body, lowering the overall level.
What is hyponatremia in medicine?
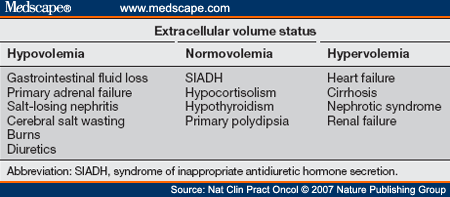
Drug and Medication Use. Treatment. References. Hyponatremia is an important electrolyte abnormality with the potential for significant morbidity and mortality. Common causes include medications and the syndrome of inappropriate antidiuretic hormone (SIADH) secretion. Hyponatremia can be classified according to the volume status ...
What is hyponatremia in nursing home?
Hyponatremia generally is defined as a plasma sodium level of less than 135 mEq per L (135 mmol per L). 1, 2 This electrolyte imbalance is encountered commonly in hospital and ambulatory settings. 3 The results of one prevalence study 4 in a nursing home population demonstrated that 18 percent of the residents were in a hyponatremic state, and 53 percent had experienced at least one episode of hyponatremia in the previous 12 months. Acute or symptomatic hyponatremia can lead to significant rates of morbidity and mortality. 5 – 7 Mortality rates as high as 17.9 percent have been quoted, but rates this extreme usually occur in the context of hospitalized patients. 8 Morbidity also can result from rapid correction of hyponatremia. 9, 10 Because there are many causes of hyponatremia and the treatment differs according to the cause, a logical and efficient approach to the evaluation and management of patients with hyponatremia is imperative.
What is SIADH in urology?
SIADH is a diagnosis of exclusion and should be suspected when hyponatremia is accompanied by urine that is hyperosmolar compared with the plasma . This situation implies the presence of a low plasma osmolality with an inappropriately high urine osmolality, although the urine osmolality does not necessarily have to exceed the normal range. Another suggestive feature is the presence of hypouricemia caused by increased fractional excretion of urate. 29 Common causes of SIADH are listed in Table 3.
What causes hyponatremia in patients?
In these patients, the main causes of hyponatremia are renal disorders, endocrine deficiencies, reset osmostat syndrome, syndrome of inappropriate antidiuretic hormone secretion (SIADH), and drugs or medications. Because of their prevalence and importance, SIADH and drugs deserve special mention, and the author will elaborate on these causes later ...
How much saline should I use for hyponatremia?
Acute severe hyponatremia (i.e., less than 125 mmol per L) usually is associated with neurologic symptoms such as seizures and should be treated urgently because of the high risk of cerebral edema and hyponatremic encephalopathy. 32 The initial correction rate with hypertonic saline should not exceed 1 to 2 mmol per L per hour, and normo/hypernatremia should be avoided in the first 48 hours. 33 – 35
Why is SIADH important?
SIADH is an important cause of hyponatremia that occurs when normal bodily control of antidiuretic hormone secretion is lost and anti diuretic hormone is secreted independently of the body’s need to conserve water. Antidiuretic hormone causes water retention, so hyponatremia then occurs as a result of inappropriately increased water retention in the presence of sodium loss. The diagnostic criteria for SIADH are listed in Table 2. 28
How to know if you have hyponatremia?
Most patients with hyponatremia are asymptomatic. Symptoms do not usually appear until the plasma sodium level drops below 120 mEq per L (120 mmol per L) and usually are nonspecific (e.g., headache, lethargy, nausea). 11 In cases of severe hyponatremia, neurologic and gastrointestinal symptoms predominate. 3 The risk of seizures and coma increases as the sodium level decreases. The development of clinical signs and symptoms also depends on the rapidity with which the plasma sodium level decreases. In the event of a rapid decrease, the patient can be symptomatic even with a plasma sodium level above 120 mEq per L. Poor prognostic factors for severe hyponatremia in hospitalized patients include the presence of symptoms, sepsis, and respiratory failure. 12
How to treat hyponatremia?
If you have mild symptoms, your doctor makes small adjustments to your therapy to correct the problem. This usually involves restricting water intake, adjusting medications and removing or treating the causes.
What is the best medication for hyponatremia?
Certain newer medications, like tolvaptan (Samsca®), may be used to correct blood sodium levels. Treatment to correct any underlying medical problems – like congestive heart failure (when poor heart function causes fluid to build up in the body) – is also used to improve hyponatremia.
What is hyponatremia in labs?
What is hyponatremia? Hyponatremia is usually discovered on laboratory tests as a lower than normal sodium level in the blood. It will appear as sodium or Na+ in your lab results. Actually, the main problem in the vast number of situations is too much water that dilutes the Na+ value rather than too much sodium.
Why is hyponatremia a problem?
What causes hyponatremia? In general, too much water in your body is usually the main problem and this dilutes the sodium levels. Much less frequently, hyponatremia is due to significant sodium loss from your body. Too much water in your body causes your blood to become “watered down.”.
What happens if you have hyponatremia?
In many cases, hyponatremia causes extra water to move out of the bloodstream and into body cells, including brain cells. Severe hyponatremia causes this to occur quickly, resulting in swollen brain tissue. If left untreated, complications can include: 1 Mental status changes 2 Seizures 3 Coma 4 Death
Can you lose too much sodium?
It’s also possible to lose too much sodium from your body. Medications, like diuretics, can cause your kidneys to increase the amount of sodium excreted in urine. Medical problems like diarrhea may cause excessive sodium loss if left untreated. Chronic or binge alcohol consumption can cause people to lose too much sodium through increased urination and vomiting. You can have hyponatremia without feeling dehydrated or volume depleted. This is most often the case in hospitalized patients.
Can you get hyponatremia after surgery?
Anyone can develop hyponatremia. Hyponatremia is more likely in people living with certain diseases, like kidney failure, congestive heart failure, and diseases affecting the lungs, liver or brain. It often occurs with pain after surgery.
Overview

Symptoms
Causes
Risk Factors
Complications
Prevention
- Hyponatremia treatment is aimed at addressing the underlying cause, if possible. If you have moderate, chronic hyponatremia due to your diet, diuretics or drinking too much water, your doctor may recommend temporarily cutting back on fluids. He or she may also suggest adjusting your diuretic use to increase the level of sodium in your blood. If you...