Wilson’s T3 protocol is aimed at depleting T4 and RT3 levels in the tissues of the body, for a time, hopefully allowing the converting enzyme to come back up to normal. This is accomplished by reducing TSH
Thyroid-stimulating hormone
Thyroid-stimulating hormone is a pituitary hormone that stimulates the thyroid gland to produce thyroxine, and then triiodothyronine which stimulates the metabolism of almost every tissue in the body. It is a glycoprotein hormone produced by thyrotrope cells in the anterior pituitary gland, which regulates the endocrine function of the thyroid. In 1916, Bennett M. Allen and Philip E. Smith found that the pituitary …
Does Wilson's T3 therapy work?
This appears to be what enables the patients’ thyroid systems to function well on their own again. Wilson’s T3 therapy does not need to be taken for life, rather usually only a few weeks or months. Another common feature of T3 therapy involves cycling the patient on and off T3 therapy.
What medications are used to treat Wilson's disease?
If you take medications for Wilson's disease, treatment is lifelong. Medications include: Penicillamine (Cuprimine, Depen). A chelating agent, penicillamine can cause serious side effects, including skin and kidney problems, bone marrow suppression, and worsening of neurological symptoms.
What are the most common features of T3 therapy?
Another common feature of T3 therapy involves cycling the patient on and off T3 therapy. There’s something about weaning a patient off T3 and starting it again that often helps them break through periods of stagnation in their treatment progress (possibly by reducing resistance to T3 therapy).
How can I manage Wilson's disease on a daily basis?
Lifestyle and home remedies. If you have Wilson's disease, your doctor will likely recommend that you limit the amount of copper you consume in your diet. You might also want to have your tap water's copper levels tested if you have copper pipes in your home. And be sure to avoid multivitamins that contain copper.
What is Wilson's T3 protocol?
Denis Wilson. The WT3 protocol involves the use of SR-T3 taken orally by the patient every 12 hours according to a cyclic dose schedule determined by patient response. The patient is then weaned once a body temperature of 98.6 degrees F has been maintained for 3 consecutive weeks.
What are the symptoms of Wilson's temperature syndrome?
The diagnostic criteria for Wilson's syndrome — low body temperature and nonspecific signs and symptoms, such as fatigue, irritability, hair loss, insomnia, headaches and weight gain — are imprecise.
Can Wilson's disease symptoms come and go?
The signs of Wilson's disease can be mild and may come and go over months or years, or they may be ongoing. Half of all patients have their first symptoms due to deposits of copper in the brain and nervous system. These symptoms include: Speech and language problems.
How do you test for Wilson's temperature syndrome?
The main diagnostic sign is an oral body temperature that averages well below 37.0 °C (98.6 °F). This overlaps with normal body temperature, which is usually within the range of 36.5–37.5 °C (97.7–99.5 °F). Wilson says that his diagnosis is confirmed if the patient responds to treatment with slow-release T3 (SR-T3).
What happens if T3 is not done properly?
If T3 therapy is not done properly, patients can waste a lot of time and money (on visits and medicine) without even knowing it . We use the term Wilson’s T3 Therapy (the WT3 protocol) to distinguish our protocol from other ways doctors give T3 medicine.
Does WT3 affect body temperature?
In many cases the symptoms of MED have been seen to be almost inseparably related to body temperature patterns. The WT3 protocol can often very effectively, predictably, reproducibly, and comfortably influence body temperature patterns.
Is WT3 a therapeutic protocol?
So the WT3 protocol can be useful as a symptomatic (addressing the symptoms) and/or a therapeutic (correcting the underlying problem) intervention for the symptoms of MED due to low body temperature patterns especially when due to Wilson’s Temperature Syndrome.
WTS Treatment
Sluggishness, poor concentration, assorted aches and pains—most of us experience these symptoms from time to time. If they persist or grow severe, we want a diagnosis quickly so we can find some relief. With thousands of accepted medical diagnoses, however, pinpointing the precise cause of our problems can be a challenge.
Liothyronine (T3) Treatment
The T3 medicine that is currently on the market (Cytomel) is instant release. But Dr. Wilson and other doctors prefer using T3 that has been mixed with a sustained-release agent for Wilson’s T3 therapy. This appears to be best accomplished by skilled and experienced pharmacists with specialized equipment.
What is Wilson's disease?
Wilson's disease also is associated with a type of cataract, called a sunflower cataract, that can be seen on an eye exam.
How to test liver for Wilson's disease?
Liver biopsy is commonly performed by inserting a thin needle through your skin and into your liver. Diagnosing Wilson's disease can be challenging because its signs and symptoms are often hard to tell from those of other liver diseases, such as hepatitis.
What tests can be done to diagnose Wilson's disease?
Genetic testing. A blood test can identify the genetic mutations that cause Wilson's disease. Knowing the mutations in your family allows doctors to screen siblings and begin treatment before symptoms arise.
What to ask for when making a Wilson's appointment?
When you make the appointment, ask if there's anything you need to do in advance, such as restrict your diet for blood tests. Make a list of: Your symptoms and when they began. Key personal information, including major stresses, other medical conditions you have and any family history of Wilson's disease.
How long does it take for T3 to be depleted?
Thus, even though it is often hard for the patients to hold off chasing the temperature with T3 for the 10 days T4 and RT3 levels are being depleted, it’s important for them to know that by doing so, they can often be as far along in 3 weeks as they otherwise might be in six months if they don’t.
How long should I stop T4?
If the patient’s on .075 mg of T4, I might stop the T4 in one step if the patient does not appear to be brittle (a clinical judgment). Otherwise, I might cut the dose in half for two days and then discontinue it. If the patient’s on around .3mg, I might recommend going down a third (.1 mg) every 2 days until it is discontinued. Generally, the less constitutionally resilient a patient appears to be (again clinical), the more gradually I wean the T4-containing medicine. However, I don’t usually like to go any more slowly than I have to, because the longer it takes to wean the patient off the T4, the longer it will be before the 10 day period begins, and I don’t want the treatment to take unnecessarily long. Also, I am not very concerned about the patient weaning off the T4 because I know we’ll have T3 “waiting in the wings” to come in and support the patient if necessary.
How long does it take to cycle off T4?
And cycling on and off the medicine takes time (each cycle can take over a month). By weaning the T4-containing medicine first patients are often able to capture their temperatures on much lower dosages of T3, thereby saving them as much as six months worth of therapy.
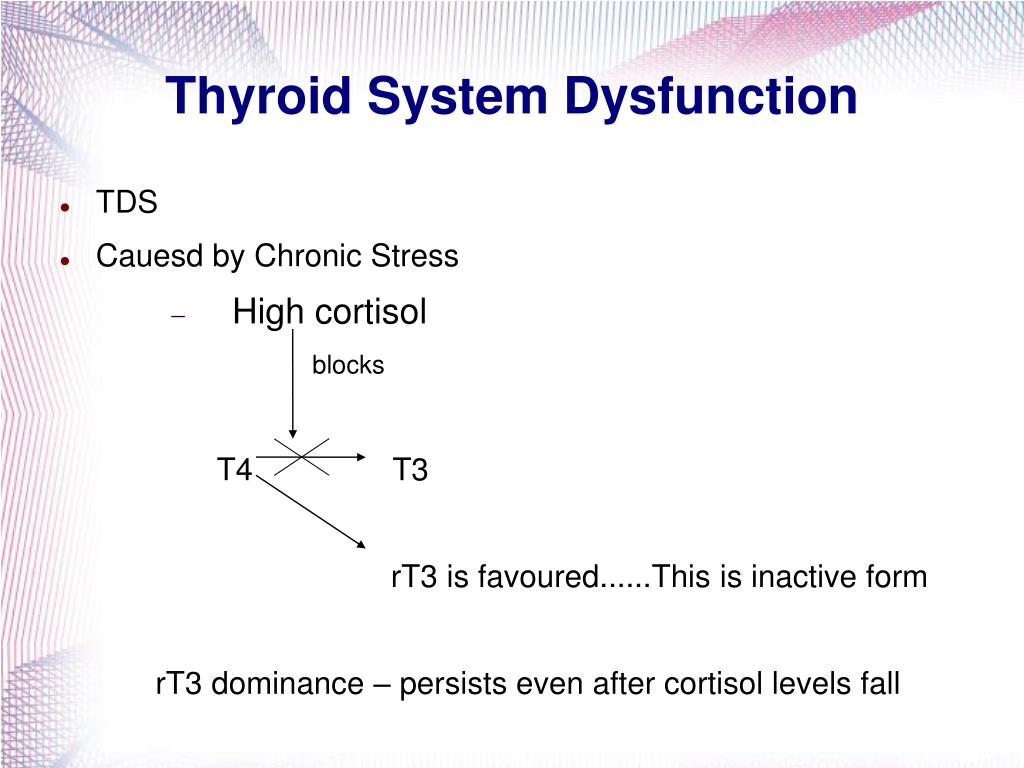
Does T4/RT3 compete with T3?
If there is a T4/RT3 preponderance the T4 certainly, and perhaps the RT3 to a smaller extent, will compete with any exogenous T 3 administered at the site of the nuclear membrane receptors in the cells. So from the start, more T3 will be needed to generate the same amount of thyroid stimulation of the cell than would be needed if there was no T4/RT3 ...
Can Wilson's temperature syndrome cause low thyroid?
But the symptoms of low thyroid system function are more commonly caused by Wilson’s Temperature Syndrome, not hypothy roidism. People diagnosed as hypothyroid who are taking T4-containing medicine may never have been hypothyroid, or if they were, may not be now. By hypothyroid I mean those patients who actually have low thyroid gland function.
Is T3 more dependent on T4 or T3?
This is because a patient’s T3 supply is more dependent on T4 to T3 conversion by the deiodinating enzyme when the patient is taking some T4. Given these observations, some might wonder if it would be better to leave hypothyroid patients on T3 therapy, rather than to put them back on T4. Not usually.
Can T3 therapy be increased?
To repeat, for that 10 day period the T3 therapy is not to be increased (or started) in an attempt to raise the patients’ temperatures and to improve the patients’ symptoms, but only as needed to support the patients clinically, to prevent a worsening of their symptoms.