Chemotherapy vesicant & irritant properties and suggested management for extravasation
| Drug | Vesicant or Irritant | Apply Heat or Cold | Additional treatment/antidote |
| Aclarubicin (Aclacinomycin) | Irritant | Cold (different suggestions for anthracy ... | (off-label, based on general management ... |
| Ado-trastuzumab emtansine (Kadcyla) | Irritant | Cold - 15 to 20 minutes at a time for at ... | None known |
| Amsacrine (Amsidine) | Vesicant | Cold - 15 to 20 minutes at a time for at ... | None known |
| Arsenic trioxide (Trisenox) | Irritant | Cold - 15 to 20 minutes at a time for at ... | None known |
What is a vesicant drug?
If the medication is a vesicant drug — meaning that it has the potential to cause tissue damage through blistering and ulceration — doctors call this complication extravasation. Vesicants include several chemotherapy drugs.
How do you administer vesicant drugs safely and effectively?
- Secure the cannula during the administration of the drug. - Even if there is an existing IV route, secure a new route when administering vesicant drugs. - If in doubt, re-insert the cannula and administer the drug. - Watch for edema, inflammation, and pain around the cannula during administration.
What is extravasation of a vesicant?
Introduction Extravasation of a vesicant is a potentially disfiguring event associated with many commonly used intravenous antineoplastics. There are numerous reports of paclitaxel causing tissue damage including blistering following extravasation [Stanford and Hardwicke, 2003].
Are chemotherapeutic agents vesicants?
Some chemotherapeutic agents, such as the vinca alkaloids and the anthracyclines, are universally accepted as vesicants with well-described physicochemical properties and supportive literature detailing the consequences of extravasation.

What are current recommendations for treatment of drug extravasation?
Warm compresses are preferred for extravasation of specific drugs including vinca alkaloids, etoposide, vasopressors, and oxaliplatin to increase local blood flow and enhance drug removal. Apply compresses for 20 to 60 minutes 3 or 4 times daily for the first 24 to 72 hours after extravasation occurs.
What is a vesicant antibiotic?
Vesicants: Drugs that can result in tissue necrosis or formation of blisters when accidentally infused into tissue surrounding a vein[14]. They include Actinomycin D, Dactinomycin, Daunorubicin, Doxorubicin, Epirubicin, Idarubicin, Mitomycin C, Vinblastine, Vindesine, Vincristine, and Vinorelbine.
What is the treatment for IV infiltration?
Some possible treatments are: Elevate the site as much as possible to help reduce swelling. Apply a warm or cold compress (depending on the fluid) for 30 minutes every 2-3 hours to help reduce swelling and discomfort. Medication-If recommended, medicine for extravasations is given within 24 hours for best effect.
What is the antidote for extravasation?
MANAGEMENT OF EXTRAVASATION. *No recommended antidote. †Recommended antidote: dexrazoxane or dimethyl sulfoxide (DMSO).
How is vesicant infiltration treated?
Treatment of a vesicant extravasation includes immediate cessation of infusion, aspiration of as much extravasated drug as possible through the still-intact catheter, and attempts for the aspiration of the extravasated agent in the surrounding tissue. This aspiration may help to limit the extent of tissue damage.
How do you administer vesicant drugs?
Inject or infuse the vesicant medication through the Y-site needleless connector of a free-flowing I.V. solution, such as 0.9% sodium chloride solution. This additional fluid helps dilute the drug and reduces the risk of vein damage.
What steps will the nurse take to treat the infiltrated IV site?
TreatmentStop the infusion.Remove the IV.Mark the outline affected area with a marker.Photograph the affected area.Apply a hot or cold compress based on the type of IV fluid infiltrated.Elevate the extremity.Inject medication into the subcutaneous tissue.
What are the recommended nursing interventions when an IV becomes infiltrated?
If you are concerned an IV is infiltrated, follow your facility policy and as a general guideline, discontinue the site and relocate the IV. If the infiltration is severe, apply warm compresses, elevate the arm, monitor the site and be sure to inform the healthcare provider.
Is an infiltrated IV an emergency?
In extreme cases, IV infiltration may even result in death. If you have been injured or a loved one has died following untreated IV infiltration, you may have legal options that can help you recover damages for medical expenses and personal pain and suffering.
How do you administer phentolamine for extravasation?
Phentolamine (Regitine)2,5 Prepare by diluting 5 mg phentolamine in 10 mL of 0.9% sodium chloride. Inject subcutaneously into the extravasation area within 12 hours of extravasation. Blanching should reverse immediately; additional injections may be required if blanching returns.
Which of the following nursing actions is most important in preventing extravasation?
Limiting the pump cycle to one hour may minimise the extent of tissue damage from extravasation by triggering a reminder to inspect the insertion site and limb for signs of extravasation. Nursing vigilance along with prompt recognition and management is the key to avoiding or minimising injury.
What IV fluids are vesicants?
Some common examples of vesicant medications and fluids include vancomycin, potassium chloride, calcium gluconate, dopamine, and Dilantin.
Specific Chemical Agents
The following chemicals were chosen to represent the entire class of vesicants. Vesicants include distilled mustard (HD), mustard gas (H), mustard/lewisite, mustard/T, nitrogen mustard, sesqui mustard, and sulfur mustard.
Info for Clinicians
Case Definition: Vesicant (Mustards, Dimethyl Sulfate, and Lewisite) Includes clinical description, lab criteria for diagnosis, & case classification.
What is the difference between vesicant and extravasation?
Vesicant – an agent capable of causing blistering, tissue sloughing or necrosis when it escapes from the intended vascular pathway into surrounding tissue. Extravasation – the inadvertent infiltration of vesicant solution or medication into surrounding tissue.
When selecting an IV site, avoid areas of flexion?
1. Location, location, location : When selecting an IV site, avoid areas of flexion – this includes the wrist, hand, and antecubital fossa. Be mindful of any punctures to veins above the area you are about to stick. If patient had a recent blood draw from the antecubital fossa, use the opposite arm to find a suitable site. Oh, btw, extravasation can also happen in patients with central venous access.
What non-chemo drugs cause extravasation?
Listed below are a few non-chemo agents: Vancomycin. Nafcillin. Calcium Chloride. Potassium Chloride. Sodium Chloride. Calcium Gluconate. Dobutamine.
What is the role of contrast agents in nursing?
As nurses, it is our responsibility to take preventive measures, monitor, identify signs/symptoms and institute prompt treatment per policy or as ordered. If you administer any of these agents, prevention is key and consider the following: 1.
Can IV vesicant cause blisters?
There are several chemotherapeutic agents with vesicant properties, and when inadvertently infused into the surrounding tissue from an infiltrated IV, these agents may have the potential to cause blisters, severe tissue injury or necrosis, known as extravasation.
Can an IV pump tell if an IV site is infiltrating?
Infusion pumps will not tell you if an IV site in infiltrating. Always aspirate for positive blood return prior to use, but remember, checking for blood return or back flow of blood is good for patency but not a reliable method for assessing infiltration at IV site.
Is it better to use a small IV catheter or a large IV catheter?
2. Bigger is not better: Use the smallest gauge IV catheter to administer the prescribed therapy. Good flow rates are possible even with a small gauge catheter. Using an IV catheter too large for the vein will obstruct blood flow and might cause thrombosis distal to the IV site. 3.
Pathophysiology
Sulfur mustard and nitrogen mustard alkylate many cellular components, including DNA, and also release inflammatory cytokines. They have similar acute local effects on the skin, eyes, and airways; at lethal concentrations, they suppress bone marrow.
Symptoms and Signs
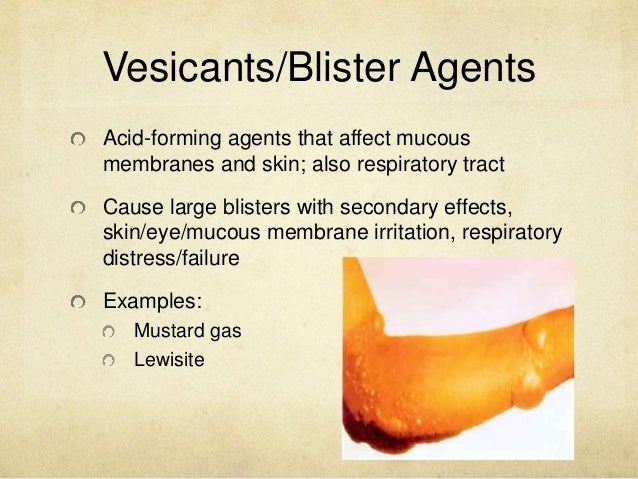
Mustard compounds cause intense and increasing skin pain, erythema, and blister formation after a latent period. The latent period is inversely correlated with dose but is usually at least a few hours (and up to 36 hours).
Diagnosis
Pain occurring at or shortly after exposure suggests that Lewisite or phosgene oxime is the agent; the early onset of skin changes distinguishes phosgene oxime. Delayed onset of pain (sometimes until a day after exposure) suggests sulfur mustard.
What are vesicants and irritants?
Vesicants are chemicals that cause blistering of the skin or mucous membranes [Polovich et al. 2009]. Irritants cause tissue inflammation or irritation without associated blister formation, and local effects of irritant extravasation resolve with minimal intervention [Polovich et al. 2009]. Two mechanisms of tissue injury following extravasation of vesicants have been proposed. The first involves initial DNA damage with poly (ADP-ribose) polymerase activation, subsequent nicotinamide adenine dinucleotide (NAD+) depletion leading to glycolysis inhibition, and cellular protease cleavage of adherent fibrils connecting the basal epidermal cell layer to the basement membrane [Papirmeister et al.1985]. The second mechanism involves local glutathione depletion leading to a loss of protection from free radicals, particularly those involved in lipid peroxidation, with direct tissue damage as a result [Gentilhomme et al. 1992]. Neither mechanism has been specifically linked to taxanes.
Is chemotherapeutic agent a vesicant?
However, these professional organizations neither designate chemotherapeutic agents as vesicants or irritants nor recommend specific sites of administration for particular agents. In contrast, the Chemotherapy and Biotherapy Guidelines and Recommendations for Practice recommended against infusing vesicant agents peripherally for more than 30–60 min, but they also fail to categori ze specifically chemotherapeutic agents as vesicants or irritants [Polovich et al. 2009]. No current standard or scoring system exists for the classification of a compound as a vesicant, irritant, or inert compound.
Does CVAD prevent extravasation?
2009]. Administration of taxanes by CVADs does not protect from extravasation or subsequent tissue injury. More interesting is the observation that extravasation involving CVADs did not require more invasive surgical intervention for optimal control of tissue injury, as an extravasation in large, central veins could take longer to be recognized and have greater infused volumes over the same time.
Is CVAD more convenient than peripheral administration?
Although more convenient, CVAD use is associated with bloodstream infections, thrombosis, and increased cost. It is conceivable that vesicant extravasation through CVADs would be more devastating than with peripheral administration due to masking of the extent of damage. Currently there are no data to support taxane administration through CVADs versusperipheral administration to prevent extravasation or improve outcome of extravasation.
Is vesicant an antineoplastic agent?
Several classes of antineoplastic agents are universally referred to as vesicants with ample supporting literature. However, the literature surrounding the taxanes is controversial. While the American Society of Clinical Oncology and Oncology Nursing Society Chemotherapy Administration Safety Standards and the Chemotherapy and Biotherapy Guidelines and Recommendations for Practice identify the risks of extravasation and the parameters surrounding the infusion of known vesicants, recommend administration sites for known agents, and recommend antidotes for particular extravasation cases, they fail to provide specific recommendations for the administration of individual taxanes, or a classification system for antineoplastic agents as vesicants, irritants, or inert compounds. There is also a lack of prescribing information regarding such recommendations. The lack of a formal classification system further complicates the accurate delineation of vesicant antineoplastic agents and subsequent appropriate intravenous administration and extravasation management. There are several factors that make the classification of taxanes as vesicants or irritants challenging. Comprehensive preclinical data describing potential mechanisms of tissue damage or vesicant-like properties are lacking. Furthermore, most case reports of taxane extravasation fail to include the parameters surrounding administration, such as the concentration of medication and duration of infusion, making it difficult to set parameters for vesicant potential. Subsequently, many practitioners default to central venous administration of taxanes without evidence that such administration minimizes the risk of extravasation or improves outcomes thereof. Here, we review briefly the data surrounding taxane extravasation and potential vesicant or irritant properties, classify the taxanes, and propose a spectrum for antineoplastic agent potential to cause tissue injury that warrants clinical intervention if extravasation occurs.
Is vinca an anthracycline a vesicant?
Extravasation of a vesicant is a potentially disfiguring event associated with many commonly used intravenous antineoplastics. Some chemotherapeutic agents, such as the vinca alkaloids and the anthracyclines, are universally accepted as vesicants with well-described physicochemical properties and supportive literature detailing the consequences of extravasation. However, the delineation of taxanes as vesicants or irritants is poorly defined, posing a clinical controversy, and a challenge in optimal prevention and management of extravasation.
How to reabsorb extravasated vesicant?
Elevation of the limb may aid in reabsorption of the infiltrate or extravasated vesicant by decreasing capillary hydrostatic pressure. Apply sterile dressing over the area of extravasation, regularly assess the extravasation site during every shift, and take medical photographs and consult the department of cosmetic surgery if necessary.
How to stop IV fluids from extravasation?
At the first sign of extravasation, the following steps are recommended: (1) stop administration of IV fluids immediately, (2) disconnect the IV tube from the cannula, (3) aspirate any residual drug from the cannula, (4) administer a drug-specific antidote, and (5) notify the physician (Fig. 1). Open in a separate window.
What is the frequency of extravasation of drugs?
Incidence. The frequency of extravasation in adults is reported to be between 0.1% and 6%.
How often does extravasation occur in adults?
The frequency of extravasation in adults is reported to be between 0.1% and 6%. Some data suggest that the incidence is decreasing probably due to improvements in the infusion procedure, early recognition of the drug leakage, and training in management techniques.
What is extravasation in medicine?
Extravasation refers to the leakage of injected drugs from blood vessels causing damage to the surrounding tissues. Common symptoms and signs of extravasation include pain, stinging or burning sensations, and edema around the intravenous (IV) injection site.
What are the items required for extravasation?
Documentation procedure may differ between treatment centers (documentation form); however, certain items are mandatory for patient safety and legal purposes: (1) patient name and number, (2) date and time of the extravasation, (3) name of the drug extravasated and the diluent used (if applicable), (4) signs and symptoms (also reported by the patient), (5) description of the IV access, (6) extravasation area (and the approximate amount of the drug extravasated), and (7) management steps with time and date.
When to report extravasation of chemo?
Patients must be informed to report any changes in sensation, signs, or symptoms during the IV administration of any chemotherapeutic drug and to alert the healthcare professionals to early signs of extravasation. Particular information must be given when a vesicant drug is administered. Extravasation must be suspected if any of the following specific signs or symptoms are presented (Table 1).
What happens when a vesicant leaks out of the vein and into the surrounding tissue?
Extravasation occurs when a vesicant drug leaks out of the vein and into the surrounding tissue. When this happens, a person will likely experience serious tissue damage, including ulceration and tissue death, if they do not receive treatment in time.
What is the term for the process of destroying tissue and seeping out of veins?
Extravasation occurs when IV medications, which can destroy tissue, seep out of veins and into the surrounding skin and muscle.
Why does extravasation decrease?
However, improvements in infusion techniques and a higher awareness among healthcare professionals of the early signs of extravasation are causing the rate to decrease. Extravasation has many possible causes, including: repeatedly using the same veins for cannulation. fragile veins.
How severe is extravasation?
The severity of extravasation depends on how much medication has entered the surrounding tissue and how strongly the tissue reacts to the medication. Very severe cases of extravasation could result in the loss of limb tissue or function.
What happens when you take a venous cannula?
When a healthcare professional administers a drug through a venous cannula, there is a small risk of the solution leaking out of the veins and into the surrounding tissue. If the medication is a vesicant drug — meaning that it has the potential to cause tissue damage through blistering and ulceration — doctors call this complication extravasation. ...
Why does an IV line get extravasated?
Extravasation may occur if the administration of the drug is too quick, the medication is very acidic or basic, or there is an obstruction in the intravenous (IV) line .
How long after stopping a syringe can you monitor your skin?
The medical team will continue to monitor the skin for 24 hours after stopping the infusion to check for signs of infection.