Is low-density lipoprotein cholesterol the best target for Lipid Management in CHD patients?
Oct 13, 2020 · 4.2 In adults with type 1 diabetes with chronic kidney disease in stages 1–4, we suggest statin therapy, irrespective of the cardiovascular risk score, to reduce cardiovascular risk. (2⊕OOO) Technical Remarks: Low-density lipoprotein should be the primary target for lipid-lowering therapy.
What is the 2020 guideline on Lipid Management in endocrine disorders?
Abstract. Lipid management in primary and secondary prevention reduces cardiovascular morbidity and mortality. Lowering of low-density lipoprotein cholesterol (LDL-C) levels with statins remains the primary goal of therapy. For secondary prevention patients, those with coronary heart disease (CHD) or CHD risk equivalents, intensive LDL-C lowering is recommended, although the …
What is the primary target for lipid-lowering therapy?
Overview of Clinical Guidelines in Lipid Management. www.lipid.org. Primary Objective. • Outline current guidelines on the management and treatment of patients with dyslipidemia. www.lipid.org. ATP I. • LDL-C primary target: – High risk >160 mg/dL or ≥130 mg/dL and 2 or more risk factors (RFs)– <130 mg/dL considered desirable • HDL-C considered a major RF but …
What are the current cholesterol management guidelines?
Hence LDL-C has been considered as the primary target of cholesterol lowering efforts. It has been observed that statins, the cholesterol-lowering drugs, dramatically reduce heart attacks, CHD deaths, and overall mortality rates with lowering of LDL-C. [ 3]
What is the primary target when using medication to lower lipids?
What is the primary target of treatment in lipid management LDL TG HDL cholesterol?
ATP III recommends that LDL cholesterol be the primary target of therapy. The LDL cholesterol goals for each risk category are shown in Table IV. 1-1. LDL-C goal for multiple-risk-factor persons with 10-year risk >20 percent = <100 mg/dL.Dec 17, 2002
What is the most important target of therapy to improve a lipid profile?
9 LDL cholesterol remains the primary target of therapy; however, treatment beyond LDL cholesterol lowering is recommended for men and women with triglyceride levels at or above 200 mg per dL (2.26 mmol per L).Jan 15, 2002
What is the primary treatment for hyperlipidemia?
What is the target LDL?
What is the treatment goals in the management of hyperlipidemia?
What is lipid treatment?
Which of the lipids are considered to be a target in dyslipidemia treatment?
What is the management of lipid disorder?
What is primary hyperlipidemia?

What is the nursing intervention for hyperlipidemia?
| Hyperlipidemia Nursing Interventions | Rationale |
|---|---|
| Provide supplemental oxygen as necessary. | To improve cardiac function, reduce ischemia, and lower lactic acid production, increase the amount of oxygen available for myocardial absorption. |
What is the main cause of hyperlipidemia?
What is the role of cholesterol in the cell membrane?
Cholesterol, an integral component of cell membranes and a precursor for bile acids and steroid hormones, travels in the blood with the help of proteins called lipoproteins . There are three major classes of lipoproteins: Low density lipoprotein (LDL), high density lipoprotein (HDL), and very low-density lipoprotein (VLDL), which typically constitutes 60-70%, 20-30%, and l0-15% of the total cholesterol, respectively. As LDL-C binds to maximal concentration of cholesterol, it can be considered as a mirror image of total cholesterol concentration in blood. Hence LDL-C has been considered as the primary target of cholesterol lowering efforts. It has been observed that statins, the cholesterol-lowering drugs, dramatically reduce heart attacks, CHD deaths, and overall mortality rates with lowering of LDL-C.[3]
What databases are used to search for cholesterol?
We identified electronic databases, mainly MEDLINE, HighWire, Cochrane and Google Scholar for searching articles from 1980 through February, 2012 by using keywords “Cholesterol Management Guidelines,”, “National Cholesterol Education Program”, “Adult Treatment Panel”. In MEDLINE, we have used “(cholesterol) AND (Adult treatment panel) AND (Guidelines)” as the Medical Subject Heading (MeSH) terms.
What is the ATP IV?
The ATP-IV guideline would be using markers like Apo B, non-HDL-C (non-LDL-C markers) and tailored-treatment approach (personalized or individualized care) in making therapeutic decisions. This tailored-treatment approach was based more directly on clinical trial evidence than treat-to-target paradigm and may potentially translate into better outcomes in terms of patient management, at the same time reduce harm and cost of the therapy incurred by over-treating low-risk/low benefit individuals.[40,41] In this approach, the intensity of statin therapy was based on an individual's overall five to 10-year cardiovascular risk irrespective of LDL level which saved approximately 100,000 more quality-adjusted life years per annum, leading to a lower number of patients on high statin dose/s. Furthermore, it showed unexpected high effectiveness or efficiency than treat-to-target approach that even 10 international lipid experts, who strongly supported an LDL-based approach were not able to provide any scientific rationale to use treat-to-target approach.[42] Summarizing, the new ATP-IV guideline would preferably use tailored-treatment approach and promise to align its recommendations with strong clinical evidence regarding cardiovascular risk and risk reduction with lipid lowering agents, especially the statins and would also help in minimizing over-and under-treatment and in promoting optimized treatment with statin therapy.
What is the ATP III guideline?
The adult treatment panel-III, comparatively a recent ATP guideline was supported by evidence from continuing research and widespread consensus on the benefits of aggressive treatment of high blood cholesterol.[6] The ATP-III guideline provided evidence based strategies for identifying and reducing CHD risk.[21] The most distinctive feature of ATP-III that differentiated it from ATP I and ATP II guideline was introduction of the concept of risk and risk assessment as the first step in risk management strategies, considering both long-term (lifetime) and short-term (10-year) risks. According to this guideline, it was important to identify a lifetime risk in people who were relatively at low short-term risk but had a single major-risk factor. This helped to identify apparently healthy individuals even with a single aberrant risk factor. It also emphasized on exhaustive risk lowering strategies (especially drug therapies) in patients with higher short-term risk while exhaustive TLC was considered for patients with higher lifetime risk of cardiovascular diseases (CVD).[22]
What is ATP cholesterol?
Adult Treatment Panel (ATP), an expert panel to supervise cholesterol management was set up under the aegis of National Cholesterol Education Program (NCEP) in 1985. Since then NCEP-ATP has been revising and framing guidelines to enable clinician to deliver better treatment to cardiovascular patients and to educate general people. As a result, considerable reduction in cardiovascular related deaths has been observed in recent times. All three ATP guidelines viz. ATP-I, ATP-II and ATP-III have targeted low density lipoprotein as their primary goal. The ATP-III guideline was updated in the light of evidences from 5-major clinical trials and was released in 2004. It added therapeutic lifestyle changes, concept of risk equivalents, Framingham CHD-risk score non-high density lipoprotein cholesterol (non-HDL-C) as secondary target and gave strong emphasis on metabolic risk factors. The earlier treat-to-target paradigm faced fierce criticism from clinicians across the globe because of insufficient proof of safety and benefits of treating patients with respect to an individual's low density lipoprotein (LDL) level. Further, demonstration of non-HDL-C and total cholesterol/HDL-C ratio as strong predictors of overall cardiovascular risk foresees new guidelines. A tailored-treatment approach was suggested instead of LDL-C target based treatment approach which was soundly based on direct clinical trials evidences and proposes treatment based on individual's overall 5- to 10-year cardiovascular risk irrespective of LDL-C level, leading to lower number of people on high dose/s of statins. Recent report of the Cholesterol Treatment Trialist's Collaborators meta-analysis strongly supported primary prevention of LDL with statins in low risk individuals and showed that its benefits completely outweighed its known hazards. Markers other than LDL-C like apolipoprotein B, non-HDL-C and total cholesterol/HDL-C ratio would take precedence in the risk assessment and strong emphasis would be given on tailored-treatment approach in the upcoming ATP-IV guideline.
What is step 2 in CHD?
Step II: Identification of the presence of atherosclerotic disease that heightens the risk for CHD events (CHD risk equivalent) e.g. clinical CHD, symptomatic carotid artery disease, peripheral arterial disease and abdominal aortic aneurysm.
What is the step VIII of TLC?
Step VIII: Identification of metabolic syndrome, and treat, if present, after three months of TLC. Treatment of metabolic syndrome included (1) treatment of underlying causes (overweight/obesity and physical activity) by intensive weight management and increased physical activity and (2) treatment of lipid/non-lipid risk factors, if persisted despite lifestyle therapies by treatment of hypertension, use of aspirin to reduce prothrombotic state in CHD patients and by treatment of elevated TG and/or low HDL (described in step IX).
How much HDL cholesterol is needed for ATP III?
The ATP III guidelines have been expanded to recognize the importance of HDL levels by raising the threshold of low HDL cholesterol from less than 35 mg per dL (0.90 mmol per L) to less than 40 mg per dL (1.05 mmol per L). [Evidence level C, consensus/expert opinion]
What is the best way to lower LDL cholesterol?
Encourages use of plant sterols/stanols as a therapeutic dietary option to lower LDL cholesterol levels
How much does a TexCAPS study increase HDL cholesterol?
The AFCAPS/TexCAPS study correlated a 6 percent increase in HDL cholesterol levels with a reduction of first acute major coronary events in men and women with baseline average LDL cholesterol levels and below-average HDL cholesterol levels.
How often should I check my cholesterol?
Screening is still recommended for all patients 20 years or older and every five years thereafter. The lipoprotein profile cannot be interpreted without knowledge of the patient's risk factors. Risk factor counting remains an important part of the guidelines ( Table 2). 4 In ATP III, diabetes is no longer on this risk factor list but is now included in a new category termed “CHD risk equivalent.”
How much cholesterol is high?
High HDL cholesterol (> 60 mg per dL [1.55 mmol per L]); presence of this risk factor removes one risk factor from the total count
When did the NCEP ATP III guidelines come out?
In May 2001, the NCEP–ATP III released its third set of guidelines, reflecting changes in calculating coronary risk and in the management of hypercholesterolemia. According to the new guidelines, the number of patients with cholesterol levels that can be classified as abnormal has now tripled.
Why is cardiovascular risk reduction important for women?
Cardiovascular disease is the primary cause of death among American women, far exceeding the rate of all cancers combined. 1 Women's mortality following myocardial infarction is three times that of men, 8 suggesting that women may not be active participants in cardiovascular risk reduction strategies. By demonstrating cardiovascular event reduction through the use of statins, the 4S, CARE, and AFCAPS/TexCAPS trials support cholesterol-lowering therapy in women. [Evidence level A, RCTs/meta-analyses]
What is the best way to classify lipid metabolism disorders?
The best way of classifying lipid metabolism disorders is descriptively (Table 3), based on the changes in concentration of the various types of lipids. LDL hypercholesterolemia is distinguished from mixed hyperlipoproteinemia, hypertriglyceridemia, and an isolated reduction in HDL cholesterol. All these disorders of lipid metabolism can be associated with elevated lipoprotein(a). The treatment of the individual lipid metabolism disorders is described below.
How long does it take to follow up on lipid lowering medication?
Before treatment with lipid-lowering medications; follow-up 4–6 weeks after beginning of treatment, then only in event of clinical symptoms
How can evidence be translated into concrete recommendations for patient management?
How the collected evidence can be translated into concrete recommendations for patient management is currently the subject of intensive debate. The national and international professional societies are in agreement that: 1 The focus should be on high-risk patients with proven atherosclerosis or multiple risk factors 2 Lifestyle modification measures are of great importance 3 Statin-based lowering of LDL cholesterol plays a pre-eminent part in medicinal treatment
Why are statins used in medicine?
Statins play a predominant role in medicinal treatment due to the positive results of endpoint studies.
What is the most common disorder of lipid metabolism in diabetics?
Mixed hyperlipoproteinemia. Owing to its close association with the metabolic syndrome, mixed hyperlipoproteinemia, in which the concentrations of both LDL cholesterol and triglycerides are raised, is the most frequently occurring disorder of lipid metabolism in diabetics (35).
What are the disorders of lipid metabolism?
The main disorders of lipid metabolism are LDL-hypercholesterolemia, hypertriglyceridemia, mixed hyperlipoproteinemia, and low HDL cholesterol. The lipoprotein(a) level can also be elevated either in isolation or in combination with other disorders of lipid metabolism.
Does lowering LDL cholesterol lower cardiovascular risk?
Altogether, the available data permit the conclusion that lowering of LDL cholesterol leads to a decrease in the rate of cardiovascular events. Whether this applies to all LDL cholesterol-lowering approaches remains open, but the answer is probably affirmative (at least for measures that lead to swifter elimination of LDL cholesterol from the plasma).
How long after initiation of lipid lowering medication should you monitor?
Patients on lipid-altering agents should be monitored 4-12 weeks after initiation or dose adjustment and then at least annually to assure adherence to the drug and lifestyle. Statin intolerance is defined as the inability to tolerate at least two different statins, including at least one at the lowest starting dose. The accuracy of low levels of LDL-C, particularly when the triglycerides are elevated, is better estimated by the Martin/Hopkins than with the Friedewald equation.
What drugs are used to lower LDL-C?
Several new agents are in clinical trials including an oral nonstatin inhibitor of ATP citrate that up-regulates LDL receptor activity as do other LDL-C lowering drugs; longer-acting PCSK9 inhibitors; and anti-sense drugs targeting Lp (a), angiopoietin-like 3, lipoprotein lipase, and apo C-3, each of which has the potential for decreasing ASCVD events beyond that attributable to lowering the LDL-C.
What is the LDL C of a diabetic?
In persons with severe hypercholesterolemia defined as an LDL-C ≥190 mg/dl, high-intensity statin therapy is recommended. If the LDL-C remains ≥100 mg/dl, consideration should be given to ezetimibe, a PCSK9 inhibitor, or both. Similarly, in patients with diabetes, there is no need to use the risk calculator.
Is LDL-C lower than ASCVD?
There is a correlation between LDL-C and ASCVD and recent evidence supports the concept of “lower is better,” with the magnitude of event reduction proportional to the degree of LDL-C lowering. For every 39 mg/dl reduction in LDL-C, there is a >20% reduction in ASCVD events and 10% reduction in all-cause mortality. Considering the benefit of lowering LDL-C increases with the increasing risk, the focus for treatment is to identify persons at greatest risk of CVD and to treat with high-intensity statins.
What are the 2018 and 2019 guidelines for individualized cholesterol management?
The documents address more detailed risk assessment, newer nonstatin cholesterol-lowering drugs, special attention to patient subgroups, and consideration of the value of therapy, all with the aim of creating personalized treatment plans for each patient. Overall, the guidelines recommend shared decision-making to meet the individual needs of each patient.
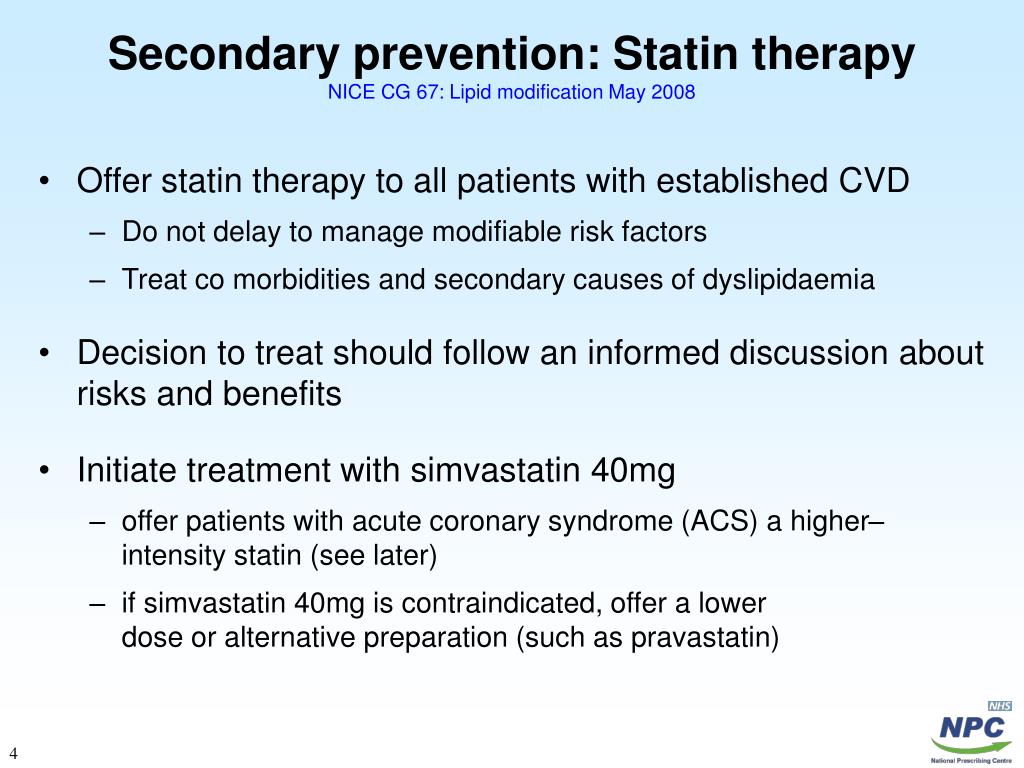
What is statin therapy?
In addition to a heart-healthy lifestyle (which should be encouraged for all patients across their life course), statins are the foundation of lipid management. Statin therapy is divided into 3 categories of intensity: High-intensity, aiming for at least a 50% reduction in LDL-C. Examples:
How does PCSK9 affect LDL-C?
PCSK9 inhibitors lower LDL-C by 50% to 60% by binding to PCSK9, inhibiting labeling of LDL receptors for degradation, thus prolonging LDL receptor activity at the cell membrane. Several trials showed that PCSK9 inhibitors reduce cardiovascular risk in patients with stable atherosclerotic cardiovascular disease or recent acute coronary syndromes who are already on moderate- or high-intensity statin therapy. 4, 6, 7
What is the ACC/AHA recommendation for atherosclerotic cardiovascular disease?
The ACC/AHA guidelines state in a class IIA recommendation that race and ethnicity influence the risk of atherosclerotic cardiovascular disease and the choice of treatment. Risk varies widely among and within ethnic groups, affecting treatment decisions ( Table 3 ). 14 – 18 In particular, the guidelines point out that South Asian individuals have higher risk, as do those who identify as Native American or Alaskan native compared with non-Hispanic white populations. 14
What is the purpose of statins?
Statins are the foundation of pharmacologic therapy, to which ezetimibe and, if necessary, a proprotein convertase subtilisin/kexin type 9 inhibitor can be added to achieve lipid goals.
What is class I recommendation?
The guidelines award classes of recommendations, signifying the certainty of benefit compared with the estimated risk and the strength of the recommendation. Class I (strong)—benefit greatly exceeds risk; treatment is recommended. Class IIa (moderate)—benefit exceeds risk; treatment is reasonable.
Does Ezetimibe lower LDL cholesterol?
Ezetimibe decreases cholesterol absorption and consequently lowers LDL-C levels by about 20%. A large randomized trial in patients who recently had acute coronary syndromes showed that ezetimibe modestly reduced cardiovascular risk over 7 years of follow-up when added to their regimen of moderate-intensity statin therapy. 4, 5
How often should you repeat LDL C?
Assess patient adherence and the percentage response to LDL-C–lowering medications and lifestyle changes with a repeat lipid measurement 4-12 weeks after initiation of statin therapy or dose adjustment; repeat every 3-12 months as needed.
Is cholesterol a risk factor for cardiovascular disease?
An elevated total cholesterol or low density lipoprotein (LDL) cholesterol level and/or a reduced high density lipoprotein (HDL) cholesterol level are traditional risk factors for cardiovascular disease (CVD); when cholesterol elevations occur in combination with other risk factors, a much higher risk for CVD is predicted. Risk algorithms include lipid levels with some combination of the following other traditional risk factors:
