What inhalers are available for the treatment of COPD?
Trelegy Ellipta is the only FDA approved COPD inhaler in the United States that contains three separate, long-acting medications in one inhaler: fluticasone, an ICS, umeclidinium, a LAMA and vilanterol, a LABA. Working together, these medications reduce bronchoconstriction, open your airways, reduce inflammation and improve lung function.
What is the best treatment for COPD?
Surgery
- Bullectomy. COPD can destroy the air sacs in your lungs. ...
- Lung volume reduction surgery. COPD causes lung damage, which also plays a role in breathing problems. ...
- Endobronchial valve surgery. This procedure is used to treat people with severe emphysema. ...
- Lung transplant. Some people with severe COPD eventually need a lung transplant. ...
- Pulmonary rehab. ...
What medication is used for COPD?
Unit-dose vials of Arformoterol Tartrate Inhalation Solution are indicated for the long-term maintenance treatment of bronchoconstriction in patients with chronic obstructive pulmonary disease (COPD), including chronic bronchitis and emphysema. Arformoterol Tartrate Inhalation Solution can be administered through solely nebulization to the patient.
What is the best COPD medication?
What is an inhaler and how does it work?
- Types of inhalers. You may hear your provider refer to an inhaler as a “preventer” or “reliever.” These terms refer to the type of medication in the inhaler.
- Spacer chambers. When you are prescribed an inhaler, you may also be prescribed a spacer. ...
- Nebulizers. ...
What is the most important pharmacologic treatment for symptom relief in COPD?
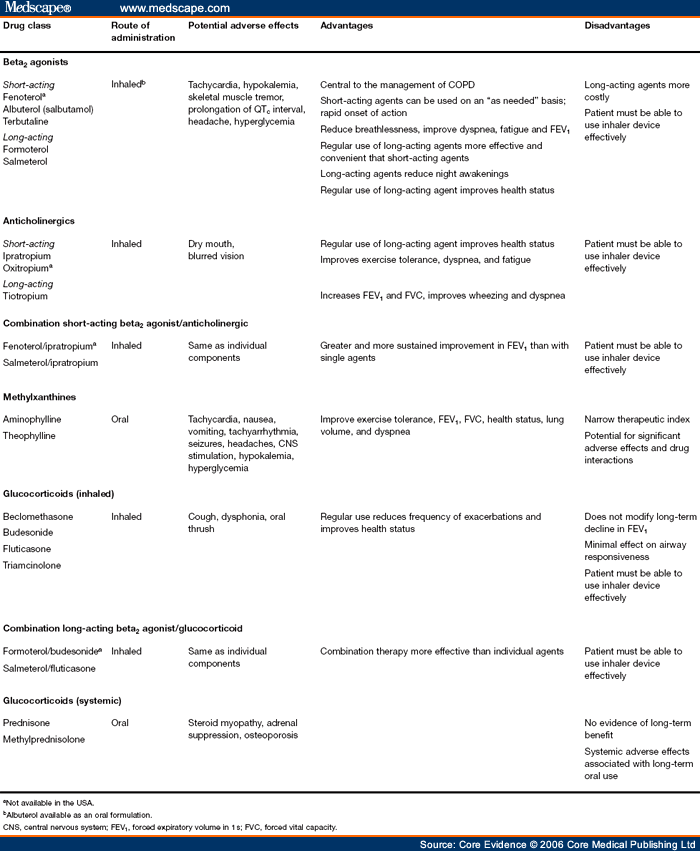
The mainstays of drug therapy for stable symptomatic COPD are inhaled bronchodilators (beta agonists and muscarinic antagonists) given alone, in combination, or with addition of inhaled glucocorticoids.
What are some common pharmacological and non pharmacological treatments for COPD?
The mainstay of pharmacological therapy is bronchodilators, while non-pharmacological methods include smoking cessation, pulmonary rehabilitation, immunizations and long term oxygen among others.
What are 2 non pharmacological treatment for COPD?
Non-pharmacologic treatments include supplemental oxygen, cigarette cessation, nutritional support and others. In addition, several new pharmacologic agents with novel mechanisms of action in early stages of development may be of potential benefit to COPD patients including those in acute exacerbation.
What types of drugs treat COPD?
They include:Albuterol and ipratropium (Combivent Respimat; Duoneb)Budesonide and formoterol (Symbicort)Fluticasone and salmeterol (Advair)Fluticasone and vilanterol (Breo Ellipta)Formoterol and mometasone (Dulera)Tiotropium and olodaterol (Stiolto Respimat)Umeclidinium and vilanterol (Anoro Ellipta)More items...•
What are some non pharmacologic methods that can be used to relieve pain?
Non-Drug Options for Easing PainMassage. A lot of people find relief from gentle massage, and some hospice agencies have volunteers who are trained in massage therapy. ... Relaxation techniques. ... Acupuncture. ... Physical therapy. ... Pet therapy. ... Gel packs.
What are two non-pharmacological things you could do to improve breathing and open airway?
Non-pharmacologic Treatment Respiratory interventions can include cooling through fan therapy,4 water spray,5 or changing the room environment, or interventions such as supplemental oxygen or compressed air.
What is the best treatment for COPD?
For most people with COPD, short-acting bronchodilator inhalers are the first treatment used. Bronchodilators are medicines that make breathing easier by relaxing and widening your airways. There are 2 types of short-acting bronchodilator inhaler: beta-2 agonist inhalers – such as salbutamol and terbutaline.
What is a non-pharmacological?
Non-pharmacological pain therapy refers to interventions that do not involve the use of medications to treat pain. The goals of non-pharmacological interventions are to decrease fear, distress and anxiety, and to reduce pain and provide patients with a sense of control.
What is oxygen therapy for COPD?
Long-term oxygen therapy has been shown to help COPD patients who have severely low blood oxygen. This therapy involves breathing in oxygen through a nasal tube or mask. NIH-funded scientists set out to determine if this same treatment would also help COPD patients who had moderately low blood oxygen.
What medications therapies and or other treatments are used to control COPD?
MedicationsBronchodilators. Bronchodilators are medications that usually come in inhalers — they relax the muscles around your airways. ... Inhaled steroids. ... Combination inhalers. ... Oral steroids. ... Phosphodiesterase-4 inhibitors. ... Theophylline. ... Antibiotics.
What is the newest treatment for COPD?
There's also a triple inhaled therapy for COPD that combines three long-acting COPD medications. The first approved triple inhaled therapy for COPD was called fluticasone/umeclidinium/vilanterol (Trelegy Ellipta). In 2020, the FDA approved a second: budesonide/glycopyrrolate/formoterol fumarate (Breztri Aerosphere).
What medications are given for COPD exacerbation treatment?
Mild to moderate exacerbations of COPD are usually treated with older broad-spectrum antibiotics such as doxycycline, trimethoprim-sulfamethoxazole and amoxicillin-clavulanate potassium.
What is the objective of COPD?
The objective of pharmacological treatment of chronic obstructive pulmonary disease (COPD) is to prevent and control symptoms, reduce the frequency and severity of exacerbations, and improve general health status and exercise tolerance. None of the classes of drugs currently used in the treatment of COPD are able to modify the progressive decline in lung function which is the hallmark of this disease (Anthonisen et al 1994; Pauwels et al 1999; Vestbo et al 1999; Burge et al 2000). Smoking cessation is currently the only intervention which has been shown to reduce the progression of COPD (GICOPD 2001). To achieve this objective, behavioral therapy and pharmacological treatment such as the administration of bupropion (an antidepressant), and nicotine replacement therapy have proved useful (Jorenby et al 1999; Tashkin et al 2001). However, it is important to try to control symptoms of COPD with pharmacological treatment using the following general proposals (GICOPD 2001): 1 There should be a stepwise increase in treatment, according to the severity of the disease. The step-down approach used in the chronic treatment of asthma is not applicable to COPD. 2 Treatment needs to be chronic and maintained at the same level for long periods of time, unless significant side effects or exacerbations occur. 3 Since individual patient response to the pharmacological treatment is variable, it is important to monitor pharmacological treatment closely and, if necessary, adjust it frequently.
What is the objective of pharmacological treatment of chronic obstructive pulmonary disease?
The objective of pharmacological treatment of chronic obstructive pulmonary disease (COPD) is to prevent and control symptoms, reduce the frequency and severity of exacerbations, and improve general health status and exercise tolerance.
What is an exacerbation of COPD?
According to a recent definition, exacerbations of COPD are “a variation in symptoms above the normal day to day variation which causes a change in a patient’s medication ” (Rodriguez-Roisin 2000). Exacerbations of COPD worsen general health status (Seemungal et al 1998) and are considerably expensive.
Is antimuscarinic bronchodilator better for asthma?
The effectiveness of antimuscarinic drugs depends on the role that cholinergic vagal tone has in the pathophysiology of bronchial obstruction. Antimuscarinic bronchodilators are generally considered to be more effective for COPD than for asthma.
What is the best way to administer bronchodilator?
Short- and long-acting β2-agonists and antimuscarinic agents are generally administered by inhalation (aerosol, dry-powder or nebuliser solution). Bronchodilator therapy is most frequently delivered by pressurized metered-dose inhalers (MDIs) or dry-powder inhalers (DPIs).
Can glucocorticoids be used for COPD?
However, glucocorticoids are recommended for severe COPD and frequent exacerbations of COPD. New pharmacological strategies for COPD need to be developed because the current treatment is inadequate. Keywords: Chronic obstructive pulmonary disease, pharmacological treatment, bronchodilators, glucocorticoids, theophylline, antibiotics.
Can COPD be inhaled?
COPD may require inhalation of a short-acting β2-agonist on demand or, when airways obstruction is more severe, chronic administration of an antimuscarinic agent by inhalation or a long-acting β2-agonist (RS 2003). Selective β2-agonists.
What are the treatments for COPD?
COPD treatments include both medicines and other important therapies such as pulmonary rehabilitation, smoking/vaping cessation support and immunizations. If you were asked about COPD medicines you would probably think about your inhalers and you’d probably say, "they open up my lungs".
What are the two ways that medicines open up the airways in your lungs?
There are two basic ways that medicines open up the airways in your lungs: They act as Maintenance (controllers or preventers) or Relievers (rescue or quick relief). Here we’ll refer to them as either controllers or rescue relievers.
How often should I take a medicine for lung inflammation?
Medicines only work if you take them as you and your doctor or other clinician agree; that usually means at least once a day.
What is a nebulizer?
A nebulizer is a device that changes liquid medicine into a fine mist that can be inhaled into the lungs. This mist can be breathed in through a mouthpiece or face mask. There are different types of nebulizers: jet, vibrating mesh and ultrasonic nebulizers. Sometimes the vibrating mesh and ultrasonic types are lumped together under "electronic" nebulizers.
How long does a long acting beta agonist last?
Like the LAMAs, the long-acting beta agonists (also called LABAs) can last for 12 to 24 hours and so need to be taken only once or twice a day.
What is a long acting anticholinergic?
Long-acting Anticholinergic (an-tee-coe-luh-nur jick) Bronchodilators also called Long-acting Anti-Muscarinic (an tee mus car in ic) Bronchodilators (Maintenance or Controller) plus. Inside our bodies, there is a constant stream of messages being sent to keep us safe and well.
Can COPD be treated?
COPD can be treated. Some treatments can decrease breathlessness, increase your ability to do activities while others may reduce your risk of exacerbations (x-saa-cer-bay-shun) (flare-ups). These treatments can make it easier for you to breathe, feel better, do more and stay out of the emergency department and hospital.
How effective are COPD medications?
Because COPD medications are effective, it is important to implement them according to the severity of the disease, the potential side effects, the tolerance of the patient for specific drugs, and their cost. Figure 4 summarizes a practical approach integrating the different available medications made on the basis of clinical and phenotypical information. Patients with features of emphysema revealed by tomography or X-ray and lung hyperinflation with low diffusion capacity, with low BMI and low eosinophils may be best treated with long-acting bronchodilators, whereas patients with features of asthma characterized by a history of allergies, wheezes, and eosinophilia may respond better to a LABA/ICS combination. At each medical visit, check for development of side effects, inquire about adherence, and ascertain whether the patient is using the inhalers correctly because incorrect use is highly prevalent and a reason for therapeutic failure.
What causes COPD to die?
After a long subclinical phase, once symptoms develop, COPD frequently follows a course of worsening dyspnea at ever lower effort and progressive gas exchange imbalance, with death occurring from respiratory failure or from associated comorbidities such as coronary artery disease and lung cancer. 10. McGarvey L.P.
Is COPD a bronchodilator?
Most are antiinflammatory in nature with little bronchodilator effect; their benefit is measured using outcomes such as exacerbation and health status.
Does smoking cessation affect lung function?
The effect of pharmacotherapy on disease progression has been considered minimal, whereas the myth persists that only smoking cessation modifies the accelerated decline of lung function of COPD. This is not so. First, close to one-half of patients receiving a diagnosis of GOLD stage II COPD after age 60 have no evidence of accelerated decline of FEV 1
Is COPD undertreated?
In addition, variations in health plan coverage for the many medications required by individuals who frequently suffer from several comorbidities, and misunderstanding the benefit of therapy, conspire to make COPD a major disease that remains totally undertreated.
Can bronchodilator be used after hospitalization?
Their use should be considered only in individual patients with symptoms after hospitalizations for COPD on adequate bronchodilator therapy or who have been treated with systemic corticosteroids during their admission.
Abstract
Chronic Obstructive Pulmonary Disease (COPD) is currently the 4th leading cause of death worldwide but is projected to be the 3rd leading cause of death by 2020. In Portugal, the estimated prevalence of COPD in the Lisbon region is 14.2%, and a large proportion of underdiagnosed disease has been detected.
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is currently the 4th leading cause of death worldwide but is projected to be the 3rd leading cause of death by 2020.1 In Portugal, the estimated prevalence of COPD in the Lisbon region is 14.2%, and a large proportion of underdiagnosed disease has been detected. 2
Conclusions
Based on the GOLD 2017/2018 and on new evidence that has emerged regarding treatment options with the FLAME study, this paper provides an update on a previous proposal for pharmacological treatment approaches to COPD patients.
Financial support
Funding for this paper was provided by Novartis Portugal. Funding was used to access all necessary scientific bibliography and cover meetings expenses. Novartis Portugal had no role in the collection, analysis and interpretation of data, in the writing of the paper and in the decision to submit the paper for publication.
Conflicts of interest
Nuno Pires reports personal fees from Novartis. Paula Pinto reports personal fees from Novartis. Nelson Marçal reports personal fees from Novartis, Teva and Boehringer-Ingelheim. António Jorge Ferreira reports personal fees from Novartis, Bial, Boehringer-Ingelheim, GSK, Tecninfar and Teva. Cidália Rodrigues reports personal fees from Novartis.
How to get rid of COPD?
Exercise. This is also important when you have COPD. It helps increase your stamina and strengthens the muscles that help you breathe. Your doctor or physical therapist can help you design a fitness program that's safe for you.
How does COPD affect oxygen levels?
Severe COPD can prevent you from getting enough air into your lungs. As a result, oxygen levels in your blood can get too low. Therapy increases these levels to help you stay active and healthy. You breathe in oxygen through a mask or prongs in your nose.
What is the procedure to remove air spaces in the lungs?
A bullectomy is surgery to remove the air spaces and improve the flow of air in your lungs. Lung volume reduction surgery. The surgeon removes small pieces of your lungs that COPD has damaged. Removing the damaged parts helps the healthy parts of your lungs expand so they can take in more oxygen.
What is the name of the tiny pouches in your lungs where oxygen travels into your blood vessels?
Air sacs are the tiny pouches in your lungs where oxygen travels into your blood vessels. COPD destroys the walls of these air sacs. When the walls come down, they create large spaces in your lungs called bullae. These bullae make it hard to breathe.
How to improve stamina and breathlessness?
These techniques, combined with a physical exercise program , can help lessen breathlessness and increase stamina.
Does Theophylline help with COPD?
Theophylline can help your lungs work better, but it may not control all of your symptoms. Antibiotics. An infection can make your COPD symptoms worse. Your doctor will give you antibiotics to kill the bacteria and treat the infection. Take all the medicine you're prescribed.
Can you use COPD machines at home?
People with moderate to severe COPD may use these machines at the hospital to help with sudden, intense symptoms or at home to help with sleep and to keep blood oxygen levels up and remove carbon dioxide. Just remember that regular use of these machines isn’t always helpful for COPD.
What is the mainstay of COPD treatment?
Bronchodilators are the mainstay of the current pharmacological management of COPD. Long-acting bronchodilators reduce exacerbations and improve health-related quality of life [ 6 – 11 ].
What is the goal of COPD?
The two main goals of the current management of chronic obstructive pulmonary disease (COPD) are: 1) to reduce the impact of the disease on daily activities; and 2) to reduce the risk of future events (exacerbations, lung function decline and death) [ 1 ].
How does emphysema affect the respiratory system?
It can lead to incapacitating dyspnoea by destruction of alveoli, decrease in the surface area available for gas exchange, as well as pulmonary hyperinflation altering the mechanical properties of the respiratory system . These modifications in pulmonary mechanical forces and their subsequent effects on the inflammatory cascade are thought to play a key role in disease progression [ 87 ]. In recent years, studies have shown that dynamic as well as static hyperinflation can significantly contribute to dyspnoea in subjects with emphysema [ 87, 88 ]. Smoking cessation, inhaled bronchodilators and corticosteroids, and home oxygen therapy offer certain benefits in emphysema but a majority of patients remain symptomatic despite optimal medical therapy. Since the beginning of the 20th century, a variety of surgical approaches and techniques have been described to improve function and/or survival in patients with emphysema [ 89 ]. Currently, only three procedures may be considered, namely bullectomy, lung volume reduction surgery (LVRS) and lung transplantation [ 89 ]. Ideally, each of these procedures would have specific indications, leading to individualised tailoring of surgery. In reality, there is a large degree of overlapping of indications, and several candidates could be suitable for more than one procedure. In fact, there is a continuum of lesions between giant bullae, heterogeneous emphysema and homogeneous emphysema. Similarly, functional improvement following bullectomy and LVRS share some mechanisms. In this section, a brief review of literature concerning bullectomy and LVRS will be provided.
Why is integrated care important for COPD?
Because COPD is a complex, multi-domain disease, integrated care programmes are considered essential to provide the best care possible [ 39 ]. The precise structure of this type of programmes is not yet universally defined but most probably should include education (improving the inhaler technique as well as adherence to therapy) and a programme to stimulate regular physical activity, as well as the measures aimed at improving the coordination among levels of care or the responsiveness of care that may allow earlier recognition and treatment of exacerbations [ 40 – 44 ]. Underuse, overuse and improper use are the most common causes of poor adherence to COPD therapy. On average, 40–60% of patients with COPD adhere to the prescribed regimen and only one out of 10 patients with a metered dose inhaler performs all essential steps of device handling and drug inhalation correctly [ 40 ]. A strong association between increased adherence and improved all-cause mortality and reduction in hospital admission, independent of study treatment, has been reported in the TORCH study [ 45 ]. New bronchodilators, either ultra-long-acting β 2 -agonists such as indacaterol or long-acting antimuscarinic agents administered on a once daily basis, may improve compliance since this regimen is preferred by most patients [ 46 ]. Some of these new bronchodilators are also developed as combinations of either an ultra-long-acting β 2 -agonists and a long-acting antimuscarinic or an ultra-long-acting β 2 -agonists and a corticosteroid.
What is roflumilast used for?
Roflumilast is the first specific inhibitor of phosphodiesterase-4 in the process of being marketed in COPD to treat severe patients with bronchitic symptoms and a history of exacerbations . In recently published trials, roflumilast modestly improved lung function and mainly reduced the rate of moderate to severe exacerbations independently of concomitant use of long-acting bronchodilators [ 36, 37 ]. Other clinical studies are required to clarify the place of this agent in the range of drugs available for COPD [ 38 ].
Is COPD more prevalent in females than males?
COPD prevalence is progressively increasing in females and studies have suggested a poorer outcome in females than males. E kstrom et al. [ 68] extended this research to severe COPD patients requiring LTOT and found higher relative mortality for females compared with males, both overall and related to respiratory disease, cardiovascular disease and cancer. C oleta et al. [ 69] showed that readily available parameters, such as dyspnoea intensity and hypoxia severity, may be useful in predicting first-year survival rates in advanced COPD patients receiving LTOT. Hypercapnia is also associated with a poor prognosis, but F remault et al. [ 70 ], in a small physiological study, showed that inspired fraction of CO 2 did not increase markedly during controlled oxygen therapy using either a facial mask (O 2 10 L·min −1) or nasal prongs (2 L·min −1 ). These data were generated on a short-term basis and should probably be tested in larger populations to identify possible subgroups of responders and nonresponders.
Is LTOT good for COPD?
Another important, and still unsolved, issue is the possible benefits of LTOT in COPD patients who are normoxic at rest but who desaturate during physical activity. The National Heart, Lung and Blood Institute workshop suggested a comparison of oxygen versus room air in such patients. A recent systematic review of 31 randomised controlled studies in 534 patients receiving oxygen or room air provided evidence that oxygen during exercise improves endurance, maximal exercise capacity and breathlessness in patients with moderate to severe COPD [ 60 ]. There seemed to be more inconsistent results in patients with diurnal Pa,O2 >60 mmHg. However, the clinical relevance of these short-term improvements is still unclear as tests in the laboratory may not reflect the physical activity in daily life. There is a clear need to study patients in their homes and daily environment.
