Explore
Feb 10, 2005 · For patients with newly diagnosed deep vein thrombosis (DVT), good evidence indicates that outpatient treatment is safe and effective using low-molecular-weight heparin and an oral anticoagulant until the international normalized ratio (INR) is in therapeutic range.
What is the life expectancy with portal vein thrombosis?
Jan 01, 2007 · This chapter reviews the conventional treatment of venous thromboembolism. Deep vein thrombosis (DVT) and pulmonary embolism (PE) can be considered manifestations of the same clinical entity, venous thromboembolism (VTE). The objectives of the treatment of patients with VTE are to prevent postthrombotic syndrome, recurrent VTE, and death from PE.
How to treat thrombosis naturally?
May 17, 2018 · Superficial vein thrombosis, or SVT, is a blood clot in a vein located close to the surface of the skin. Like deep vein thrombosis (or DVT), SVT often results in inflammation in the affected vein, though its symptoms are usually much more conspicuous. It affects as many as 125,000 Americans, many of whom also suffer from varicose veins.
What is treatment for non occlusive thrombus?
Oct 24, 2006 · Abstract. Deep-vein thrombosis (DVT) is a common condition that can lead to complications such as postphlebitic syndrome, pulmonary embolism and death. The approach to the diagnosis of DVT has evolved over the years. Currently an algorithm strategy combining pretest probability, D-dimer testing and compression ultrasound imaging allows for safe ...
What causes blood clots in surface veins?
Portal vein thrombosis (PVT) is the most frequent among the splanchnic vein thrombosis, accounting for 90% of cases. More than half of PVT are provoked by liver cirrhosis, solid cancer or myeloproliferative neoplasms. The remaining cases are non-malignant non-cirrhotic PVT and include either unprovo …
What is the typical treatment for deep vein thrombosis?
What is first line treatment for a deep vein thrombosis?
What are the types of thrombosis and treatment?
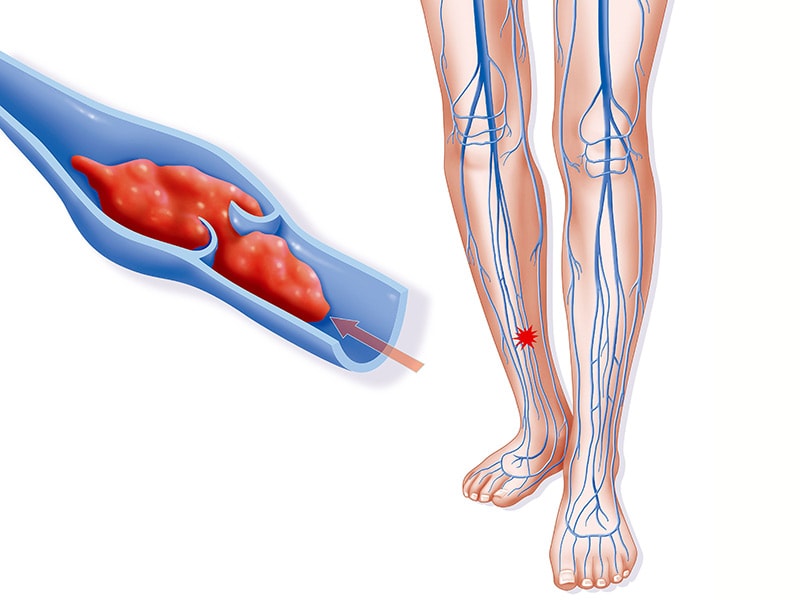
- Venous thrombosis is when the blood clot blocks a vein. Veins carry blood from the body back into the heart.
- Arterial thrombosis is when the blood clot blocks an artery. Arteries carry oxygen-rich blood away from the heart to the body.
What is conservative treatment for DVT?
Which doctor will treat DVT?
How long should DVT treatment last?
Can thrombosis be cured?
What causes vein thrombosis?
What is the difference between a blood clot and thrombosis?
Do you treat non occlusive thrombus?
Will a CT scan show a blood clot in the leg?
What are the side effects of oral anticoagulants?
The major side effect of oral anticoagulant therapy is bleeding. 70, 87, 88 A number of risk factors have been identified that predispose to bleeding on oral anticoagulants. 88, 89, 90 The most important factor influencing bleeding risk is the intensity of the INR. 87, 88, 89, 90 Other factors include a history of bleeding , previous history of stroke or myocardial infarction, hypertension, renal failure, diabetes, and a decreased hematocrit. 89 Efforts have been made to quantify the bleeding risk according to these underlying clinical factors. 89, 90 Introduction of a multicomponent intervention combining patient education and alternative approaches to the maintenance of the INR resulted in a reduced frequency of major bleeding in the patients in this group. 89 Furthermore, patients in the intervention group were within the therapeutic INR a significantly greater amount of time than were patients in the standard care group. In a retrospective cohort study of patients with an INR greater than 6.0, it was shown that a prolonged delay in the return of the INR to the therapeutic range was seen in patients who had an INR over 4.0 after two doses of warfarin were withheld, patients with an extreme elevation of the INR, and older age patients, particularly those with decompensated congestive heart failure and active cancer.90 Numerous randomized clinical trials have demonstrated that clinically important bleeding is lower when the targeted INR is 2.0 to 3.0, and that bleeding increases exponentially when the INR increases above 4.5 or 5.0. 87, 90, 91 There is a strong negative relationship between the percentage of time that patients are within the targeted INR and both bleeding and recurrent thrombosis.
What is the most commonly used test for warfarin?
The laboratory test most commonly used to measure the effects of warfarin is the one-stage PT test. The PT is sensitive to reduced activity of factors II, VII, and X but is insensitive to reduced activity of factor IX. Confusion about the appropriate therapeutic range has occurred because the different tissue thromboplastins used for measuring the PT vary considerably in sensitivity to the vitamin K-dependent clotting factors and in response to warfarin. 86, 87 Rabbit brain thromboplastin, which has been widely used in North America, is less sensitive than is standardized human brain thromboplastin, which has been widely used in the United Kingdom and other parts of Europe. A PT ratio of 1.5 to 2.0 using rabbit brain thromboplastin is equivalent to the current therapeutic range (i.e., INR 2.0 to 3.0). 86, 87 Conversely, a two- to three-fold increase in the PT using standardized human brain thromboplastin is equivalent to a 1.25- to 1.5-fold increase in the PT using a rabbit brain thromboplastin such as Simplastin or Dade-C. 86, 87
What is vitamin K?
Vitamin K is responsible for the post-translational conversion of glutamate residues into Gla in a limited number of proteins, the best known of which are the blood coagulation factors II, VII, IX, X, protein C, protein S, and protein Z, and bone matrix proteins. The best-known bone matrix proteins are osteocalcin and matrix Gla-protein (MGP).63
What is the molecular weight of heparin?
Heparin currently in use clinically is polydispersed unmodified heparin, with a mean molecular weight ranging from 10 to 16 kDa. Low molecular weight derivatives of commercial heparin have been prepared that have a mean molecular weight of 4–5 kDa. 45, 46
What are the side effects of heparin?
The main adverse effects of heparin therapy include bleeding, thrombocytopenia, and osteoporosis. Patients at particular risk of bleeding are those who have had recent surgery or trauma, or who have other clinical factors which predispose to bleeding on heparin, such as peptic ulcer, occult malignancy, liver disease, hemostatic defects, age >65 years, and female gender.
Is warfarin effective for DVT?
Patients with established DVT or PE require long-term anticoagulant therapy to prevent recurrent disease. 70 Warfarin therapy is highly effective and is preferred in most patients. Adjusted dose subcutaneous heparin or LMWH is the treatment of choice where long-term oral anticoagulants are contraindicated, such as in pregnancy or for the long-term treatment of patients in whom oral anticoagulant therapy proves to be very difficult to control. In patients with proximal DVT, long-term therapy with warfarin reduces the frequency of objectively documented recurrent VTE from 47% to 2%. 104
Can oral anticoagulant therapy be interrupted?
Patients on long-term oral anticoagulant therapy may require a temporary interruption of therapy for surgical interventions, which may vary from dental extractions to major surgery. In such cases the risk of arterial or venous thromboembolism after anticoagulants have been discontinued must be weighed against the risk of bleeding if UFH or LMWH is used for bridging anticoagulant therapy. 70, 99 In the absence of randomized clinical trials recommendations are based on large, nonrandomized cohort studies,99 which in recent years have used low-molecular-weight heparin for bridging therapy. 100, 101 These studies have shown that LMWH given in either prophylactic or therapeutic doses are effective and safe for bridging therapy. In addition this therapy is cost effective when compared with UFH in hospital. 102, 103 Thus, based on the current evidence recommendations can be made depending on the anticipated risk of thromboembolism and the risk of major bleeding with anticoagulant therapy. These recommendations range from temporary lowering of the INR for certain procedures such as dental extraction to discontinuation of oral anticoagulant therapy and bridging with either unfractionated heparin or low-molecular-weight heparin in either prophylactic or therapeutic doses until a therapeutic INR is reached post-operatively.
What is a SVT?
Here’s how you can protect yourself from this complication. Superficial vein thrombosis, or SVT, is a blood clot in a vein located close to the surface of the skin. Like deep vein thrombosis (or DVT), SVT often results in inflammation in the affected vein, though its symptoms are usually much more conspicuous.
What are the risk factors for varicose veins?
Aside from varicose veins, established risk factors include: A history of SVT or DVT. Previous experience with sclerotherapy. Pregnancy. Obesity. Regular long-distance traveling. Prolonged immobilization. SVT is also more common in women between the ages of 54-65, but it can affect anybody.
How do you know if you have SVT?
It carries with it a distinct set of symptoms, including: Pain in the affected limb. Redness and warmth in and around the vein. A palpable “cord” caused by swelling. Mild fever.
What is the best treatment for SVT?
Most cases of SVT respond well to over-the-counter remedies such as non-steroidal anti-inflammatories and compression garments. Prescription anticoagulants such as warfarin can also be effective. A recent study found that a recently developed blood thinner, fondaparinux, can reduce the risk of complications by 85%.
What causes SVT?
The causes of SVT are still unclear. While it’s historically been associated with damage to the endothelial lining and hypercoagulation, recent research suggests that it might be more closely connected to varicose veins, a condition that occurs in 62% to 70% of patients with SVT.
Does SVT require specialized treatment?
Like any vein condition, SVT requires specialized treatment. If you think you might benefit from SVT treatment, schedule an appointment with a vein specialist at the Center for Vein Restoration today to discuss your options.
Is SVT serious?
While SVT can be serious, most cases can be effectively resolved with appropriate care. A typical course of treatment is designed to alleviate symptoms, prevent them from spreading, reduce the likelihood of recurrence, and eliminate the risk of developing DVT.
What is the INR of anticoagulation therapy?
The standard intensity of oral anticoagulation therapy is an international normalized ratio (INR) of 2 to 3. In patients who have antiphospholipid antibody-related thrombosis, it has long been felt that higher intensity anticoagulation therapy is needed to prevent recurrence.48However, results of 2 randomized controlled trials showed that standard anticoagulation therapy is as effective as high-intensity treatment, even in this subgroup of patients.49,50Therefore, high-intensity anticoagulation therapy is not recommended in any patient with DVT. Maintaining good INR control will decrease the risk of postphlebitic syndrome.51There has also been debate on the usefulness of long-term low-intensity anticoagulation therapy (INR 1.5–1.9) to prevent recurrent thrombosis while reducing the risk of bleeding. A large randomized trial has shown that low-intensity anticoagulation therapy is less effective than standard anticoagulation therapy at preventing recurrent thrombosis and does not lower the risk of bleeding.52Therefore, low-intensity therapy is not recommended.
What are the risks of recurrence after stopping anticoagulation?
In addition to the thrombophilic defects described previously, 2 factors have been shown to increase the risk of recurrence after stopping anticoagulation therapy. Residual thrombosis (seen on a follow-up ultrasound scan 3 months after an initial event) increases the risk of recurrence (odds ratio 2.4).46One-third of the recurrences occur in the initially unaffected leg, which suggests that residual DVT is a marker of systemic hypercoaguability. In one study, elevated D-dimer levels 1 month after stopping anticoagulation therapy were associated with an elevated risk of recurrent thrombosis in all but cancer-related thrombosis.47However, it is unclear how to incorporate these factors into clinical decision-making. In an attempt to provide clinical guidelines, our Venous Thromboembolism Clinical Trials group (VECTOR) is conducting a study designed to create a decision rule on recurrence risk.
What is DVT in medical terms?
Deep-vein thrombosis (DVT) is a common condition that can lead to complications such as postphlebitic syndrome, pulmonary embolism and death. The approach to the diagnosis of DVT has evolved over the years. Currently an algorithm strategy combining pretest probability, D-dimer testing and compression ultrasound imaging allows for safe and convenient investigation of suspected lower-extremity thrombosis. Patients with low pretest probability and a negative D-dimer test result can have proximal DVT excluded without the need for diagnostic imaging. The mainstay of treatment of DVT is anticoagulation therapy, whereas interventions such as thrombolysis and placement of inferior vena cava filters are reserved for special situations. The use of low-molecular-weight heparin allows for outpatient management of most patients with DVT. The duration of anticoagulation therapy depends on whether the primary event was idiopathic or secondary to a transient risk factor. More research is required to optimally define the factors that predict an increased risk of recurrent DVT to determine which patients can benefit from extended anticoagulant therapy.
How common is deep vein thrombosis?
Deep-vein thrombosis (DVT) has an estimated annual incidence of 67 per 100 000 among the general population s.1,2Despite adequate therapy, 1% to 8% of patients in whom pulmonary embolism develops will die,3–5whereas others will experience long-term complications such as postphlebitic syndrome (40%)6and chronic thromboembolic pulmonary hypertension (4%).7Although anticoagulant therapy decreases the risk of recurrent thrombosis, the treatment also increases the risk of major hemorrhage. Before 1995 the approach was to image all patients with suspected DVT and to repeat tests 1 week later if results were negative.8,9This approach was inefficient, since only 10%–25% of patients with suspected DVT were found to actually have the disorder and results of serial tests were usually negative.9–12Over the last 10 years new strategies for diagnosing and treating suspected DVT have been introduced.
How sensitive is DVT ultrasound?
In many centres, ultrasound testing is limited to the proximal veins (from the common femoral vein caudally to the region of the calf veins where they join the popliteal vein), for which the sensitivity is 97%. For DVT in the calf veins the sensitivity is only 73%.13Since the distal calf is not scanned, it has been demonstrated that the ultrasound should be repeated 1 week later (serial testing) if the result is negative to detect DVT extending into the proximal veins.9However, in symptomatic patients, only 20% of thrombi detected are isolated to the calf, and only 20%–30% of these thrombi will eventually extend to the proximal venous system. (See Fig. 1for the anatomy of the deep veins of the leg.) Therefore, routine serial testing is inefficient and inconvenient. Indeed, studies using the serial testing approach have shown that only 1%–2% of patients who have a negative initial ultrasound result will be confirmed to have proximal DVT upon serial testing.13,14As a result, serial testing is not cost-effective.15,16
What is a D-dimer?
D-dimer is a degradation product of a cross-linked fibrin blood clot. Levels of D-dimer are typically elevated in patients with acute venous thromboembolism, as well as in patients with a variety of nonthrombotic conditions (e.g., recent major surgery, hemorrhage, trauma, pregnancy or cancer).19D-dimer assays are, in general, sensitive but nonspecific markers of DVT. The value of the D-dimer assay resides with a negative test result that suggests a lower likelihood of DVT, thus making it a good “rule out” test with the appropriate pretest probability. If applied properly, incorporation of D-dimer testing into diagnostic algorithms simplifies the management of a patient presenting with suspected DVT.
Can DVT be diagnosed in isolation?
Although none of the symptoms or signs of DVT is diagnostic in isolation, it has been well established that a clinical prediction rule that takes into account signs, symptoms and risk factors can be accurately applied to categorize patients as having low, moderate or high probability of DVT (Table 1). Alternatively, the same rule can be used to categorize cases as “DVT likely” or “DVT unlikely.”17Over 14 studies have demonstrated the reproducibility of this model.18Patients who are found to be at low pretest probability can have DVT safely excluded on the basis of a single negative ultrasound result.10Thus, serial ultrasound testing can be avoided in this subgroup of patients. The incorporation of plasma D-dimer testing into diagnostic algorithms can identify patients who do not require ultrasonography.17
What are the goals of endovascular therapy?
The goals of endovascular therapy include reducing the severity and duration of lower-extremity symptoms, preventing pulmonary embolism, diminishing the risk of recurrent venous thrombosis, and preventing postthrombotic syndrome.
Why is anticoagulation important?
Long-term anticoagulation is necessary to prevent the high frequency of recurrent venous thrombosis or thromboembolic events. Anticoagulation does have problems. Although it inhibits propagation, it does not remove the thrombus, and a variable risk of clinically significant bleeding is observed.
How long does anticoagulation therapy last?
Anticoagulant therapy is recommended for 3-12 months depending on site of thrombosis and on the ongoing presence of risk factors. If DVT recurs, if a chronic hypercoagulability is identified, or if PE is life threatening, lifetime anticoagulation therapy may be recommended. This treatment protocol has a cumulative risk of bleeding complications of less than 12%.
What is heparin used for?
Heparin Use in Deep Venous Thrombosis. Heparin products used in the treatment of deep venous thrombosis (DVT) include unfractionated heparin and low molecular weight heparin (LMWH) The efficacy and safety of low-molecular-weight heparin (LMWH) for the initial treatment of DVT have been well established in several trials.
What is the primary objective of deep vein thrombosis?
The primary objectives for the treatment of deep venous thrombosis (DVT) are to prevent pulmonary embolism (PE), reduce morbidity, and prevent or minimize the risk of developing the postthrombotic syndrome (PTS).
What is the most basic mechanical method for thrombectomy?
The most basic mechanical method for thrombectomy is thromboaspiration, or the aspiration of thrombus through a sheath. Mechanical disruption of venous thrombosis has the potential disadvantage of damaging venous endothelium and valves, in addition to thrombus fragmentation and possible pulmonary embolism.
Does anticoagulation reduce venous thromboembolism?
Prandoni et al found that the use of ultrasonography to determine the duration of anticoagulation can reduce recurrences of venous thromboembolism after a first episode of acute proximal DVT. In the study, 538 consecutive outpatients who had completed an uneventful 3-month period of anticoagulation were randomized to receive either fixed-duration anticoagulation (< 9 months for secondary DVT and up to 21 months for unprovoked thrombosis) or flexible-duration anticoagulation, with treatment discontinued once ultrasound showed recanalization of the affected veins. Recurrent venous thromboembolism developed in 17.2% of the patients allocated to fixed-duration anticoagulation and 11.9% of the patients allocated to flexible-duration anticoagulation; no significant difference was noted in the rate of major bleeding. [ 136]
How long does it take for a vein to close after laser treatment?
Thomas Jefferson University reports that a study of 3,000 varicose veins treated with this procedure showed that 97 percent of the vessels were still closed after 28 months. It is important to realize, however, that no treatment can prevent the development of new varicose veins.
What is endovenous laser treatment?
Endovenous laser therapy, sometimes called endovenous laser treatment, is a safe and effective procedure that treats varicose veins on an outpatient basis. According to the Stony Brook School of Medicine, these abnormal vessels affect around 40 percent of the adult U.S. population. This therapy utilizes heat from a laser to create an injury to the wall of each targeted vein, causing the vessel to close and eventually become scar tissue.
What are the problems with spider veins?
The job of these veins is transporting blood from the extremities back to the heart. When a one-way valve in a vein malfunctions, blood leaks backward into the vessel. As it pools, it causes the walls of the vein to stretch and bulge. The result of this vein health problem is the development of one of the three types of abnormal vessels.
How does ultrasound work in veins?
Once a needle is in place within the vein, the vascular specialist inserts a laser probe through it. Ultrasound imaging helps make sure that the positioning is accurate. Heat from each firing of the laser shrinks the vein until it can no longer transport blood. Neighboring healthy vessels assume the workload of the vein treated.
Can vein stripping be used for varicose veins?
Almost everybody knows someone who has suffered from varicose veins. Fortunately, use of vein stripping as the conventional treatment for these abnormal blood vessels is a thing of the past. One convenient vein treatment option vascular clinics now offer is endovenous laser therapy ( EVLT ).
Can varicose veins hurt?
Although varicose veins are often mainly a cosmetic concern, the Mayo Clinic notes that they can itch or become painful. Potential complications, while rare, include ulcers, phlebitis, bleeding, and blood clots. When conservative measures such as wearing compression stockings or shedding excess weight fail to make a patient comfortable, the alternative is eliminating these troublesome vessels.
Can you walk after a vein procedure?
Vein clinic staff members encourage patients to get up and walk soon after the procedure. Mild bruising and a feeling of tightness are common. Patients are usually able to go back to work the same day and resume their normal activities except for strenuous exertion.
What is the treatment for VTE?
Traditionally, VTE treatment is initiated with a fast-acting parenteral anticoagulant (UFH or more usually LMWH or fondaparinux) overlapping with and followed by VKA therapy (e.g. warfarin) for long-term and extended prevention of VTE recurrence. 1, 2, 22
What is the goal of VTE treatment?
The goals of VTE treatment are: Prevention of thrombus growth. Symptomatic relief.
How to reduce the burden of VTE?
The most effective and economical approach for decreasing the burden of VTE is preventing the development of DVT and PE in patients at high risk. Nevertheless, DVT and PE do occur in these patients and also sometimes develop spontaneously. Prompt diagnosis and treatment of DVT are essential to decrease the risk of recurrence, potentially fatal PE and other long-term complications.
How long does a DVT patient have to be on LMWH?
Patients with DVT/PE but without cancer should receive a NOAC in preference to a VKA for the first 3 months of treatment. Patients with DVT/PE and cancer should receive LMWH rather than a VKA or NOAC for the first 3 months.
Why should anticoagulation be used for high risk patients?
Because longer-term anticoagulation may increase the risk of bleeding, it should generally be used for patients at high risk of VTE recurrence or for specific patient subgroups.
Is dabigatran a good medicine for CrCL?
a Dabigatran is not recommended in patients with CrCl <30 ml/min. Edoxaban should be given at a dose of 30 mg once daily in patients with CrCl of 15–50 ml/min and is not recommended in patients with CrCl <15 ml/min. Rivaroxaban and apixaban are to be used with caution in patients with CrCl 15–29 ml/min, and their use is not recommended in patients with CrCl <15 ml/min
Can Rivaroxaban be administered in a single-drug approach?
Rivaroxaban and apixaban can be administered from the start of treatment in a ‘single-drug approach’, thus overcoming the complications of overlapping parenteral anticoagulant with a VKA. There is a period of intensive dosing in the acute phase of therapy – when the risk of recurrent VTE is highest 24, 25 – followed by a dose change for medium or longer-term secondary prevention.
