Explore
Treatment of Community-Acquired Pneumonia. Ampicillin-Sulbactam PLUS Azithromycin, Clarithromycin, or Doxycycline. Ceftriaxone PLUS Azithromycin, Clarithromycin, or Doxycycline Alternative but HMS Non-Preferred.
What is the difference between hospital and community acquired pneumonia?
Dec 02, 2008 · Key points Fluoroquinolones, macrolides and β-lactams are effective for the treatment of community-acquired pneumonia. Despite limited evidence, experts recommend that patients with community-acquired pneumonia be given at least 1... Severe community-acquired pneumonia should be treated with a ...
What are the most common causes of community acquired pneumonia?
1st line – oral amoxicillin, doxycycline, or a macrolide Plus – supportive care Adjunct – influenza antiviral cover with comorbidities or risk factors for drug-resistant pathogens 1st line – oral combination antibiotic therapy or fluoroquinolone monotherapy Plus – supportive care Adjunct – influenza antiviral cover inpatient VIEW ALL
What is the first line treatment for pneumonia?
Feb 01, 2006 · Consensus guidelines from ATS, 8 Infectious Diseases Society of America, 9 and Canadian Guidelines for the Initial Management of Community-Acquired Pneumonia 28 ( Figure 1 6) recommend initial...
How effective is azithromycin for treating pneumonia?
Apr 02, 2015 · During consecutive periods of 4 months, beta-lactam monotherapy, beta-lactam with a macrolide, or fluoroquinolone monotherapy was used as the preferred empirical treatment for eligible patients ...

What is the first line treatment for pneumonia?
Pneumonia should be treated with antibiotics. The antibiotic of choice for first line treatment is amoxicillin dispersible tablets. Most cases of pneumonia require oral antibiotics, which are often prescribed at a health centre.Nov 11, 2021
How do you manage community acquired pneumonia?
Patients with severe community-acquired pneumonia or who are admitted to the intensive care unit should be treated with a beta-lactam antibiotic, plus azithromycin or a respiratory fluoroquinolone.Jun 1, 2011
What is used as a second line treatment for community acquired pneumonia?
As a second-line treatment either amoxicillin/clavulanate or a second or third generation cephalosporin was most often recommended for hospitalised children (Fig.May 2, 2016
How long does it take to recover from community acquired pneumonia?
With treatment, most people improve within 2 weeks. Older adults or very sick people may need longer treatment. Those who may be more likely to have complicated pneumonia include: Older adults.
What is the drug of choice for community-acquired pneumonia?
The initial treatment of CAP is empiric, and macrolides or doxycycline (Vibramycin) should be used in most patients.Feb 1, 2006
What is the best antibiotic to treat pneumonia?
Macrolides. The best initial antibiotic choice is thought to be a macrolide. Macrolides provide the best coverage for the most likely organisms in community-acquired bacterial pneumonia (CAP). Macrolides have effective coverage for gram-positive, Legionella, and Mycoplasma organisms.
Can you take azithromycin and doxycycline together for pneumonia?
No interactions were found between azithromycin and doxycycline.
Why is azithromycin used in CAP?
Is Azithromycin Effective in the Treatment of CAP? Azithromycin may be effective in eradicating atypical organisms, but such bacteria are the causative organism in less than 20% of cases of pneumonia. The most common organism associated with CAP is Streptococcus pneumoniae.
Can doxycycline and azithromycin be taken together?
In conclusion, azithromycin combined with doxycycline was revealed to be more effective than azithromycin monotherapy in the treatment of non-gonococcal urethritis.Aug 19, 2020
How serious is community-acquired pneumonia?
Key points about community-acquired pneumonia CAP is a leading cause of death in older adults. Most healthy young adults recover from CAP without a problem. CAP can cause shortness of breath, fever, and cough. You might need to stay in the hospital to be treated for CAP.
How do you get rid of pneumonia from Covid?
Are There Treatments for COVID-19 Pneumonia? Pneumonia may need treatment in a hospital with oxygen, a ventilator to help you breathe, and intravenous (IV) fluids to prevent dehydration.Jan 25, 2022
What happens if antibiotics don't work for pneumonia?
Take all the antibiotic medicine that your doctor prescribes. If you don't, some bacteria may stay in your body. This can cause your pneumonia to come back. It can also increase your risk of antibiotic resistance.Sep 23, 2020
What are the tests for pneumonia?
Historically, common laboratory tests for pneumonia have included leukocyte count, sputum Gram stain, two sets of blood cultures, and urine antigens. However, the validity of these tests has recently been questioned after low positive culture rates were found (e.g., culture isolates of S. pneumoniae were present in only 40 to 50 percent of cases). 9 Such low positive culture rates are likely due to problems with retrieving samples from the lower respiratory tract, previous administration of antibiotics, contamination from the upper airways, faulty separation of sputum from saliva when streaking slides or plates, 9 or viral etiology. Furthermore, sputum samples are adequate in only 52.3 percent of patients with CAP, and only 44 percent of those samples contain pathogens. 10 Nonetheless, initial therapy often is guided by the assumption that the presenting disease is caused by a common bacterial pathogen.
What is pneumonia in lungs?
Pneumonia is an inflammation or infection of the lungs that causes them to function abnormally. Pneumonia can be classified as typical or atypical, although the clinical presentations are often similar. Several symptoms commonly present in patients with pneumonia.
What is CAP in healthcare?
Community-acquired pneumonia (CAP) is defined as pneumonia not acquired in a hospital or a long-term care facility.
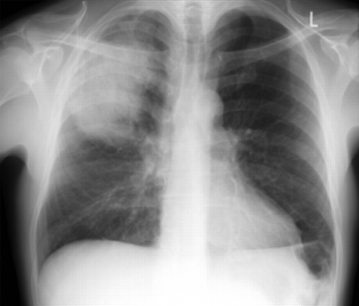
What is a chest radiograph for pneumonia?
Chest radiography (posteroanterior and lateral views) has been shown to be a critical component in diagnosing pneumonia. 8 According to the latest American Thoracic Society (ATS) guidelines for the diagnosis and treatment of adults with CAP, “all patients with suspected CAP should have a chest radiograph to establish the diagnosis and identify complications (pleural effusion, multilobar disease).” 8 Chest radiography may reveal a lobar consolidation, which is common in typical pneumonia; or it could show bilateral, more diffuse infiltrates than those commonly seen in atypical pneumonia. However, chest radiography performed early in the course of the disease could be negative.
What are the symptoms of CAP?
Common clinical symptoms of CAP include cough, fever, chills, fatigue, dyspnea, rigors, and pleuritic chest pain. Depending on the pathogen, a patient’s cough may be persistent and dry, or it may produce sputum. Other presentations may include headache and myalgia. Certain etiologies, such as legionella, also may produce gastrointestinal symptoms.
When should fluoroquinolones be used?
Respiratory fluoroquinolones should be used when patients have failed first-line regimens, have significant comorbidities, have had recent antibiotic therapy, are allergic to alternative agents, or have a documented infection with highly drug-resistant pneumococci. C. 8, 9, 28, 29.
What are the goals of pharmacotherapy for CAP?
The primary goals of pharmacotherapy for patients with CAP include eradicating the causative pathogens, resolving the clinical signs and symptoms, minimizing hospitalization, and preventing reinfection. 23 – 27 Physicians should choose a medication based on the pharmacokinetic profile, adverse reactions, drug interactions, and cost-effectiveness. 23 – 27 Further, patient evaluation should focus on severity of illness, patient age, comorbidities, clinical presentation, epidemiologic setting, and previous exposure. 9 The majority of patients with CAP are treated empirically based on the most common pathogen (s) associated with the condition. 23 – 27
What is the best medicine for pneumonia?
It may take time to identify the type of bacteria causing your pneumonia and to choose the best antibiotic to treat it. If your symptoms don't improve, your doctor may recommend a different antibiotic. Cough medicine.
How to get rid of pneumonia?
Get plenty of rest. Don't go back to school or work until after your temperature returns to normal and you stop coughing up mucus. Even when you start to feel better, be careful not to overdo it. Because pneumonia can recur, it's better not to jump back into your routine until you are fully recovered.
How long does it take for a person to feel tired after pneumonia?
Although most symptoms ease in a few days or weeks, the feeling of tiredness can persist for a month or more. Specific treatments depend on the type and severity of your pneumonia, your age and your overall health. The options include: Antibiotics. These medicines are used to treat bacterial pneumonia.
What tests are done to determine if you have pneumonia?
If pneumonia is suspected, your doctor may recommend the following tests: Blood tests . Blood tests are used to confirm an infection and to try to identify the type of organism causing the infection. However, precise identification isn't always possible. Chest X-ray.
What to do if pneumonia isn't clearing?
If your pneumonia isn't clearing as quickly as expected, your doctor may recommend a chest CT scan to obtain a more detailed image of your lungs. Pleural fluid culture. A fluid sample is taken by putting a needle between your ribs from the pleural area and analyzed to help determine the type of infection.
What is a sputum sample?
A sample of fluid from your lungs (sputum) is taken after a deep cough and analyzed to help pinpoint the cause of the infection. Your doctor might order additional tests if you're older than age 65, are in the hospital, or have serious symptoms or health conditions. These may include: CT scan.
How fast can you breathe in a minute?
Your breathing is rapid (30 breaths or more a minute) You need breathing assistance. Your temperature is below normal. Your heart rate is below 50 or above 100. You may be admitted to the intensive care unit if you need to be placed on a breathing machine (ventilator) or if your symptoms are severe.
Where was the CAP-START study performed?
The Community-Acquired Pneumonia — Study on the Initial Treatment with Antibiotics of Lower Respiratory Tract Infections (CAP-START) was performed in seven hospitals in the Netherlands, from February 2011 through August 2013 (see the Supplementary Appendix, available with the full text of this article at NEJM.org). The design and rationale of the study have been described elsewhere, 18 and the data are reported in accordance with Consolidated Standards of Reporting Trials (CONSORT) statements for cluster-randomized and noninferiority studies. 19,20 Additional study details are provided in the study protocol and statistical analysis plan, which are available at NEJM.org. The study protocol was approved by the ethics review board at the University Medical Center Utrecht (reference number 10/148), by the local institutional review boards, and by the antibiotic committee at each participating hospital.
How many patients were included in the beta lactam strategy?
A total of 656 patients were included during the beta-lactam strategy periods, 739 during the beta-lactam–macrolide strategy periods, and 888 during the fluoroquinolone strategy periods, with rates of adherence to the strategy of 93.0%, 88.0%, and 92.7%, respectively. The median age of the patients was 70 years. The crude 90-day mortality was 9.0% (59 patients), 11.1% (82 patients), and 8.8% (78 patients), respectively, during these strategy periods. In the intention-to-treat analysis, the risk of death was higher by 1.9 percentage points (90% confidence interval [CI], −0.6 to 4.4) with the beta-lactam–macrolide strategy than with the beta-lactam strategy and lower by 0.6 percentage points (90% CI, −2.8 to 1.9) with the fluoroquinolone strategy than with the beta-lactam strategy. These results indicated noninferiority of the beta-lactam strategy. The median length of hospital stay was 6 days for all strategies, and the median time to starting oral treatment was 3 days (interquartile range, 0 to 4) with the fluoroquinolone strategy and 4 days (interquartile range, 3 to 5) with the other strategies.
What is CAP in healthcare?
Introduction. Community-acquired pneumonia (CAP) is a leading cause of hospitalization and death worldwide. 1-3 Most guidelines recommend that antibiotic treatment be based on the severity of disease at presentation, assessed either on the basis of the level of care needed or on the basis of a prognostic risk score.
How long should you take antibiotics for CAP?
The recommended duration of antibiotic therapy has not changed from previously published guidelines. Patients with CAP should be treated for a minimum of 5 days, with antibiotic therapy continued until the patient achieves clinical stability.
What is CAP in pharmacy?
Community-acquired pneumonia (CAP), an infection of the lung parenchyma that occurs in persons outside ...
What is CAP in healthcare?
ABSTRACT: In 2019, guidelines for the management of immunocompetent adults with community-acquired pneumonia (CAP) were published jointly by the American Thoracic Society and the Infectious Diseases Society of America. Different treatment regimens are recommended depending on whether the patient is receiving treatment in ...
What are the causes of CAP?
The most common bacterial causes of CAP are Streptococcus pneumoniae, Haemophilus influenzae, Mycoplasma pneumoniae, Staphylococcus aureus, Legionella species, Chlamydia pneumoniae, and Moraxella catarrhalis. Although viral pathogens are becoming an increasingly common cause of CAP, the new guidelines recommend that all patients with CAP be treated empirically for bacterial infection. The basis for this recommendation is that no rapid and specific diagnostic test exists to confirm that a patient’s illness is due solely to a virus at the time of presentation, and patients with CAP caused by a virus often have a bacterial coinfection. Notably, the guidelines have eliminated the term healthcare-associated pneumonia, instead emphasizing the use of local epidemiology and risk factors to determine the need for coverage of drug-resistant pathogens, such as methicillin-resistant S aureus (MRSA) and Pseudomonas aeruginosa. 4
What are the risk factors for MRSA?
Risk factors for MRSA and P aeruginosa include prior respiratory isolation of the pathogen or hospitalization with receipt of parenteral antibiotics within the past 90 days , with locally validated risk factors for these pathogens. According to the guidelines, the process of local validation involves obtaining local data on the prevalence ...
Do macrolides prolong QT?
Both macrolides and fluoroquinolones have QT prolongation listed under the prescribing information’s warnings and precautions, and fluoroquinolones have several additional warnings, including aortic aneurysm, tendinitis or tendon rupture, peripheral neuropathy, and central nervous system effects. 6,7.
Do pharmacists work with physicians?
Pharmacists should actively work with physicians in both the inpatient and outpatient setting to ensure that patients with pneumonia receive the most appropriate antimicrobial regimen based on patient-specific factors, severity of illness, recent antimicrobial exposure, and risk of drug-resistant pathogens.
How long does it take for a patient to respond to antibiotics?
Clinical response to therapy — With appropriate antibiotic therapy, some improvement in the patient's clinical course is usually seen within 48 to 72 hours ( table 8 ). Patients who do not demonstrate some clinical improvement within 72 hours are considered nonresponders.
What is HCAP in healthcare?
Health care-associated pneumonia (HCAP; no longer used) referred to pneumonia acquired in health care facilities (eg, nursing homes, hemodialysis centers) or after recent hospitalization [ 6,7 ]. The term HCAP was used to identify patients at risk for infection with multidrug-resistant pathogens.
What is CA-MRSA?
Community-associated methicillin-resistant S. aureus (CA-MRSA) typically produces a necrotizing pneumonia with high morbidity and mortality. (See "Epidemiology, pathogenesis, and microbiology of community-acquired pneumonia in adults", section on 'S. aureus' .)
Does vancomycin reduce MIC?
One concern with vancomycin is the increasing minimum inhibitory concentrations (MICs) of MRSA that have emerged in recent years, which may reduce the efficacy of vancomycin in pulmonary infection. In patients with a MRSA isolate with an increased vancomycin MIC (≥2 mcg/mL), we prefer linezolid.
Is omadacycline FDA approved?
Omadacycline is US Food and Drug Administration (FDA) approved for the treatment of CAP and has in vitro activity against common atypical and typical CAP pathogens, MRSA, many gram-negative rods (but not Pseudomonas spp), and anaerobes [ 124,125 ].
Is CAP a serious illness?
CAP is a common and potentially serious illness [ 1-5 ]. It is associated with considerable morbidity and mortality, particularly in older adult patients and those with significant comorbidities. (See "Prognosis of community-acquired pneumonia in adults" .)

Diagnosis
Treatment
- Treatment for pneumonia involves curing the infection and preventing complications. People who have community-acquired pneumonia usually can be treated at home with medication. Although most symptoms ease in a few days or weeks, the feeling of tiredness can persist for a month or more. Specific treatments depend on the type and severity of your pne...
Clinical Trials
- Explore Mayo Clinic studiestesting new treatments, interventions and tests as a means to prevent, detect, treat or manage this condition.
Lifestyle and Home Remedies
- These tips can help you recover more quickly and decrease your risk of complications: 1. Get plenty of rest.Don't go back to school or work until after your temperature returns to normal and you stop coughing up mucus. Even when you start to feel better, be careful not to overdo it. Because pneumonia can recur, it's better not to jump back into your routine until you are fully rec…
Preparing For Your Appointment
- You may start by seeing a primary care doctor or an emergency care doctor, or you may be referred to a doctor who specializes in infectious diseases or in lung disease (pulmonologist). Here's some information to help you get ready for your appointment and know what to expect.