What is the treatment for bladder cancer?
- Surgery. If the tumor is located in the apex (i.e. top) of the bladder, a skilled surgeon may be able to remove a...
- Piroxicam. Nonsteroidal anti-inflammatory medications, especially Piroxicam, are the mainstay of treatment for TCC.
- Chemotherapy. Dogs may sometimes need chemotherapy in combination with Piroxicam or instead of...
How dangerous is bladder cancer?
The "Bladder Cancer Drug Global Market" report has been added to ResearchAndMarkets.com's offering. The Global Bladder Cancer Drug Market is estimated to be USD 3.25 Bn in 2021 and is expected to reach USD 6.89 Bn by 2026, growing at a CAGR of 16.2%.
What are the best treatment centers for bladder cancer?
Why choose Memorial Sloan Kettering for bladder cancer treatment?
- Our multidisciplinary team is among the most experienced in the field. ...
- Our surgeons are highly skilled at using advanced techniques that can limit side effects and speed recovery. ...
- Our medical oncologists specialize in chemotherapy for bladder cancer. ...
- Our radiation oncologists use advanced techniques to target areas at risk. ...
What is the latest treatment for bladder cancer?
When chemo is used without radiation, the most common combinations include:
- Gemcitabine and cisplatin
- Dose-dense methotrexate, vinblastine, doxorubicin (Adriamycin), and cisplatin (DDMVAC)
- Cisplatin, methotrexate, and vinblastine (CMV)
- Gemcitabine and paclitaxel
What are the risks of bladder cancer?
There are additional risk factors for getting bladder cancer, only some of which you can control:
- Exposure to certain chemicals, especially frequent exposure in the workplace (aniline dye and acrolein)
- Being male, Caucasian, and/or over 55
- Chronic bladder infections or irritation of the bladder lining
- Certain birth defects related to the bladder structure
- Being exposed to radiation in the past
What is the success rate of immunotherapy for bladder cancer?
Ultimately, what the study showed is that about 40 percent of patients can have their cancer eradicated with PD-1 immunotherapy, and about half of those responses last more a year.
What is the treatment for TCC?
Current treatments for transitional cell carcinoma include: Endoscopic resection, fulguration, or laser surgery. Through a ureteroscope, physicians can destroy or remove cancer cells with direct tumor removal, electrical current, or laser.
How long do you live with transitional cell carcinoma?
The median overall survival (OS) was 46 months, and the 5-year OS rate was 41.8%. The median cancer-specific survival (CSS) was 78 months, and the 5-year CSS rate was 54.3%.
Can you survive transitional cell carcinoma?
Transitional cell carcinoma of the renal pelvis, accounting for only 7% of all kidney tumors, and transitional cell cancer of the ureter, accounting for only 1 of every 25 upper urinary tract tumors, are curable in more than 90% of patients if they are superficial and confined to the renal pelvis or ureter.
Is TCC curable?
Most cases of TCC in the renal pelvis and ureter can be cured if they're found and diagnosed early enough. Surgery is the standard treatment for this type of cancer. If you need surgery, you may require a nephroureterectomy.
Is TCC painful?
Signs and Symptoms Symptoms of TCC will vary by the location of a tumor. They often resemble symptoms of a severe kidney infection wherein a person will experience painful urination and lower back/kidney pain.
What is TCC stage4?
Stage 4 is the most advanced stage of cancer. At this stage, cancer cells will usually have spread beyond the original location of the disease to other organs. Doctors consider three key factors when determining the stage of bladder cancer: size and location of the original tumor.
What is the primary symptom of transitional cell carcinoma of the bladder?
Signs and symptoms of transitional cell cancer of the renal pelvis and ureter include blood in the urine and back pain. These and other signs and symptoms may be caused by transitional cell cancer of the renal pelvis and ureter or by other conditions. There may be no signs or symptoms in the early stages.
Is transitional cell carcinoma aggressive?
Transitional Cell Carcinoma: An Aggressive Cancer This cancer may spread rapidly, affecting other organs and becoming life-threatening in some cases. Because of this, it's especially important to know more about this disease and its symptoms, as well as your treatment options at Regional Cancer Care Associates.
What causes TCC of bladder?
Factors that may increase bladder cancer risk include: Smoking. Smoking cigarettes, cigars or pipes may increase the risk of bladder cancer by causing harmful chemicals to accumulate in the urine. When you smoke, your body processes the chemicals in the smoke and excretes some of them in your urine.
Where does TCC metastasis to?
Transitional cell carcinoma (TCC) of the bladder typically metastasizes to the pelvic lymph nodes and to visceral sites including the lungs, liver, and bones. Other sites include the brain, especially after systemic chemotherapy.
Can TCC be benign?
Most TCCs of the upper urinary tract can be identified on the bases of characteristic CT appearances. However, some benign lesions may mimic different categories of TCCs and should be taken into account for differentiating diagnosis.
Where does transitional cell carcinoma metastasis?
Transitional cell carcinoma (TCC) of the bladder typically metastasizes to the pelvic lymph nodes and to visceral sites including the lungs, liver, and bones. Other sites include the brain, especially after systemic chemotherapy.
How does transitional cell carcinoma occur?
Transitional cell carcinomas arise from the transitional epithelium, a tissue lining the inner surface of these hollow organs. When the term "urothelial" is used, it specifically refers to a carcinoma of the urothelium, meaning a transitional cell carcinomas of the urinary system.
Can TCC be benign?
Most TCCs of the upper urinary tract can be identified on the bases of characteristic CT appearances. However, some benign lesions may mimic different categories of TCCs and should be taken into account for differentiating diagnosis.
How aggressive is transitional cell carcinoma in dogs?
Ultimately, TCC is a fatal disease. The tumor will most frequently grow to obstruct either the urethra or the ureters, which can result in kidney failure due to obstruction. There is also the potential for metastasis (tumor spread to a distant site).
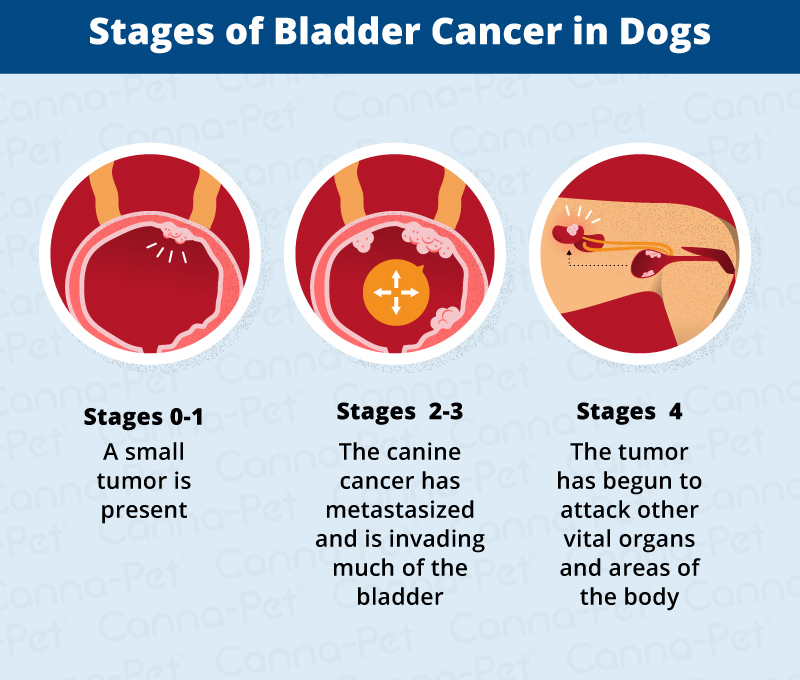
Treating Stage 0 Bladder Cancer
Stage 0 bladder cancer includes non-invasive papillary carcinoma (Ta) and flat non-invasive carcinoma (Tis). In either case, the cancer has not inv...
Treating Stage I Bladder Cancer
Stage I bladder cancers have grown into the connective tissue layer of the bladder wall but have not reached the muscle layer.Transurethral resecti...
Treating Stage II Bladder Cancer
These cancers have invaded the muscle layer of the bladder wall. Transurethral resection (TURBT) is typically the first treatment for these cancers...
Treating Stage III Bladder Cancer
These cancers have reached the outside of the bladder and might have grown into nearby tissues or organs.Transurethral resection (TURBT) is typical...
Treating Stage IV Bladder Cancer
These cancers have reached the abdominal or pelvic wall (T4b tumors) or have spread to nearby lymph nodes or distant parts of the body. Stage IV ca...
Treating Bladder Cancer That Progresses Or Recurs
If cancer continues to grow during treatment (progresses) or comes back (recurs), your treatment options will depend on where and how much the canc...
Clinical trials for TCC treatments
Developing new cancer treatments is important because different cancers and different people respond to drugs in different ways. Clinical trials are part of the process of developing new treatments. These trials can help test how safe a drug is and how well it treats that cancer. There are some new clinical trials underway to treat TCC. 1,2
Trial for chemotherapy drug combinations
Surgery is a common treatment for TCC, but it is not always completely successful. People with TCC who receive chemotherapy around the time of their surgery may survive their TCC longer. One trial, called VESPER, is comparing 2 different chemotherapy treatments given before or after surgery to remove cancer.
Trial of erdafitinib
Another trial is underway to test the safety and effectiveness of a drug called Balversa® ( erdafitinib ). This trial is studying treatments for people with metastatic or locally advanced TCC. Erdafitinib is already approved for some people with TCC who have tried all the other treatment options and still have TCC.
What is the procedure to check for TCC?
Urine cytology test to check your urine sample under a microscope for cancer cells. Procedures for diagnosing TCC include: Ureteroscopy. This is how a doctor can look inside your ureter and renal pelvis for anything that doesn’t look right.
What is the most common type of bladder cancer?
But the type of TCC that occurs in the bladder -- transitional cell carcinoma -- is the most common kind of bladder cancer. Transitional cell carcinoma can be either low grade or high grade. If it’s low grade, it isn’t likely to spread into deeper layers of your bladder or anywhere else in your body. It’s also less likely to come back ...
What is high grade bladder cancer?
High-grade TCC is the type of bladder cancer that is more likely to be life-threatening. Because transitional cells line many different parts of your urinary tract system, you can sometimes develop tumors in more than one place. If you have TCC in your bladder, you should also be checked for tumors in other parts of your urinary tract system.
What is the tube that a doctor uses to look at the kidneys?
This is how a doctor can look inside your ureter and renal pelvis for anything that doesn’t look right. They’ll use a ureteroscope -- a long, thin tube with a light on the end -- to look through your urinary system. Tissue samples can be taken during this procedure and checked for signs of disease.
What is the treatment for kidney cancer?
Surgery is the standard treatment for this type of cancer. If you need surgery, you may require a nephroureterectomy. That’s the removal of your entire kidney, ureter, and the tissue connecting the ureter to the bladder (the bladder cuff).
What is the best way to remove cancer cells from the kidney?
Segmental resection of the renal pelvis: This removes the renal pelvis where the cancer is but leaves the rest of the kidney in place. Laser surgery: A laser is used to either kill the cancer cells or remove them.
What causes transitional cell cancer?
It’s not certain what causes most transitional cell cancers, but there are certain things that can increase your risk: Being exposed to the types of industrial chemicals and dyes used to make leather products, plastics, textiles, and rubber.
What is the first treatment for bladder cancer?
Chemo (with or without radiation) is typically the first treatment when bladder cancer has spread to distant parts of the body (M1). After this treatment the cancer is rechecked. If it looks like it's gone, a boost of radiation to the bladder may be given or cystectomy might be done.
What is stage 0 bladder cancer?
Stage 0 bladder cancer includes non-invasive papillary carcinoma (Ta) and flat non-invasive carcinoma (Tis or carcinoma in situ). In either case, the cancer is only in the inner lining layer of the bladder. It has not invaded (spread deeper into) the bladder wall.
What is the treatment for T3 tumors?
An option for some patients with single, small tumors (some T3) might be treatment with a second (and more extensive) transurethral resection (TURBT) followed by a combination of chemo and radiation. If cancer is still found when cystoscopy is repeated, cystectomy might be needed.
What to do if you have cancer that hasn't been removed?
(Less often, close follow-up alone might be an option.) If all of the cancer wasn't removed, options are intravesical BCG or cystectomy (removal of part or all of the bladder).
How to get rid of stage IV cancer?
The tumor is then rechecked. If it appears to be gone, chemo with or without radiation or cystectomy are options.
How long after TA surgery can you get chemo?
For low-grade (slow-growing) non-invasive papillary (Ta) tumors, weekly intravesical chemotherapy may be started a few weeks after surgery. If the cancer comes back, the treatments can be repeated. Sometimes intravesical chemo is repeated over the next year to try to keep the cancer from coming back.
What is the treatment for cancer that recurs in distant parts of the body?
Cancers that recur in distant parts of the body can be harder to remove with surgery, so other treatments, such as chemotherapy, immunotherapy, targeted therapy, or radiation therapy , might be needed. For more on dealing with a recurrence, see Understanding Recurrence.
What are the risks of TCC?
There are a few risk factors that raise the chances of TCC including: Smoking – This increases the risk of TCC because of exposure to chemicals. The chemicals in cigarettes are passed into the urine and excreted from the body. They can damage the urinary tract and the cells, raising the risk of getting cancer.
What tests are done to check for TCC?
Cytology – The doctor may have you give a urine sample which can be looked at in the laboratory for cancer cells. X-Ray and CT Scans – Your doctor may do some imaging tests to check the urinary tract for masses.
What is the most common cancer in the urinary tract?
Transitional cell carcinoma is the most common bladder cancer. This type of cancer is in the urinary tract and affects the bladder, kidneys, and surrounding tissues and organs. TCC is also the second most common cancer that affects the kidneys accounting for up to 10 percent of urinary tract cancer.
Why do transitional cells grow?
Researchers are still unsure about the exact cause of transitional cell carcinoma. There may be a connection between smoking, infection, exposure to chemicals, and exposure to radiation. The actual cancer starts when the cell in the urinary tract begin to change and grow more rapidly than usual. The cells do not shed, but continue to grow ...
How do you know if you have transitional cell carcinoma?
The early stages of transitional cell carcinoma may not have any symptoms at all. As the cancer grows, symptoms appear including: Urinary frequency. Pain during urination. Weight loss. Severe fatigue. Lower back pain that is constant. Blood in urine.
How does a cystoscopy work?
Cystoscopy – The doctor will use a small thin tube and send it through the urethra into the bladder. There is a light and camera so your doctor can see inside the lower urinary tract.
Where does transitional cell carcinoma occur?
Transitional cell carcinoma happens in the inside lining of the bladder, the urethra, and ureters. The cells mimic regular cells and open up when the bladder is full and squeeze back together when there is nothing in the bladder. Smoking – This increases the risk of TCC because of exposure to chemicals.
What is transitional cell cancer?
Transitional cell cancer of the renal pelvis and ureter is a disease in which malignant (cancer) cells form in the renal pelvis and ureter. The renal pelvis is the top part of the ureter. The ureter is a long tube that connects the kidney to the bladder. There are two kidneys, one on each side of the backbone, above the waist.
How does chemotherapy work?
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping the cells from dividing. Biologic therapy is a treatment that uses the patient's immune system to fight cancer; substances made by the body or made in a laboratory are used to boost, direct, or restore the body's natural defenses against cancer. Regional treatment means the anticancer drugs or biologic substances are placed directly into an organ or a body cavity such as the abdomen, so the drugs will affect cancer cells in that area. Clinical trials are studying chemotherapy or biologic therapy using drugs placed directly into the renal pelvis or the ureter.
Where does cancer spread in stage 1?
In stage I, cancer has formed and has spread from the tissue lining the inside of the renal pelvis or ureter to the connective tissue layer.
Why do cancer tests have to be repeated?
Some tests will be repeated in order to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Why do we do clinical trials?
Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Can smoking cause cancer of the renal pelvis?
A personal history of bladder cancer and smoking can affect the risk of transitional cell cancer of the renal pelvis and ureter. Signs and symptoms of transitional cell cancer of the renal pelvis and ureter include blood in the urine and back pain. Tests that examine the abdomen and kidneys are used to diagnose transitional cell cancer ...
What is clinical staging of bladder cancer?
Clinical staging is based on a combination of radiographic procedures (e.g., intravenous pyelogram and computed tomographic scans) and, more recently, ureteroscopy and biopsy.
What is the prognostic factor for upper tract transitional cell cancer?
The major prognostic factor at the time of diagnosis of upper tract transitional cell cancer is the depth of infiltration into or through the uroepithelial wall.
What is the grade of transitional cell cancer?
Grade of transitional cell cancer of the upper tract has generally been found to correlate with stage. Superficial tumors are generally grade I or II, whereas the majority of infiltrative tumors are grades III and IV.
Does lymph node dissection help with nephroureterectomy?
Systematic regional lymph node dissection in conjunction with nephroureterectomy or segmental excision has not been found to enhance the effectiveness of surgery if tumors are of high grade or high stage because, in these instances, the overall results are so poor. Correspondingly, lymph node involvement is uncommon in low-stage disease, and lymphadenectomy is unlikely to remove additional tumor. Lymph node dissection at the time of nephrectomy may offer prognostic information, but little, if any, therapeutic benefit.
Is TNM staging better than tumor grade?
A TNM staging system has demonstrated accurate predictions of survival. The TNM staging system may be a better predictor of prognosis than tumor grade, although both are strongly predictive of survival. Median survival for patients with tumors confined to the subepithelial connective tissue was 91.1 months compared with 12.9 months for patients with tumors invading the muscularis and beyond, in one report. Flow cytometry analysis identifies low-stage, low-grade tumors at high risk of recurrence by virtue of their aneuploid histograms. [ 7, 8 ]
Is renal carcinoma curable?
Transitional cell carcinoma of the renal pelvis, accounting for only 7% of all kidney tumors, and transitional cell cancer of the ureter, accounting for only 1 of every 25 upper urinary tract tumors, are curable in more than 90% of patients if they are superficial and confined to the renal pelvis or ureter. Patients with deeply invasive tumors that are confined to the renal pelvis or ureter have a 10% to 15% likelihood of cure. Patients with tumors with penetration through the urothelial wall or with distant metastases usually cannot be cured with currently available forms of treatment.
Who treats bladder cancer?
Based on your treatment options, you might have different types of doctors on your treatment team. These doctors could include:
Why is it important to communicate with your cancer care team?
Communicating with your cancer care team is important so you understand your diagnosis, what treatment is recommended, and ways to maintain or improve your quality of life.
What kind of doctor treats cancer?
Based on your treatment options, you might have different types of doctors on your treatment team. These doctors could include: 1 Urologists: surgeons who specialize in treating diseases of the urinary system and male reproductive system 2 Radiation oncologists: doctors who treat cancer with radiation therapy 3 Medical oncologists: doctors who treat cancer with medicines such as chemotherapy and immunotherapy
What are the things to consider when considering cancer treatment?
Some important things to consider include: Your age and expected life span. Any other serious health conditions you have. The stage and grade of your cancer. The likelihood that treatment will cure your cancer (or help in some other way) Your feelings about the possible side effects from treatment.
What do people with cancer need?
People with cancer need support and information, no matter what stage of illness they may be in. Knowing all of your options and finding the resources you need will help you make informed decisions about your care.
What are the things to consider when making a treatment decision?
Some important things to consider include: Your age and expected life span.
What are the services offered by the American Cancer Society?
These might include nursing or social work services, financial aid, nutritional advice, rehab, or spiritual help. The American Cancer Society also has programs and services – including rides to treatment, lodging, and more – to help you get through treatment.
What is the clinical course of bladder cancer?
The clinical course of bladder tumours have a wide range of outcomes, ranging from non-muscle invasive tumours which are low-grade superficial tumours, with minimal risk of death, to, muscle-invasive tumours which are high-grade invasive tumours which are often fatal. This can be explained by the pathophysiology and oncological properties of bladder tumours. They are often described as a tumour with an implantation problem resulting in migration of the tumour to other sites, thus creating a multifocal field defect. Oncological properties also vary between different grades. Low-grade tumours have a relatively low recurrence rate and a low risk of progression; whereas, high-grade tumours have an increased propensity for malignant change and recurrence. Prognosis and long-term outcome are best predicted by the initial histological grade at the time of diagnosis, depth of invasion and the presence of Tis.15
What is the treatment for a diverticular TCC?
The gold standard of treatment for a TCC of a bladder diverticulum is radical cystectomy. Other approaches include more conservative measures, including partial cystectomy, laparoscopic diverticulectomy and TURBT, all with or without consequent intravesical chemotherapy and/or radiotherapy.16–18
What is the incidence of bladder diverticulum?
The incidence of bladder diverticula is about 1.7% and the incidence of TCC within these diverticula range from 0.8% to 13%.1–4As with bladder TCC elsewhere, the main presentation is painless hematuria. The risk factors for the development of TCC of a bladder diverticulum are those of ordinary bladder tumours, as well as those that increase the risk of developing these acquired diverticula.4As bladder diverticula lack a muscle layer and have inadequate emptying of the diverticulae, the risk of urinary tract pathologies, including urinary tract infection (UTI) and malignancies, increases.1–5
What is a diverticulae in the bladder?
Bladder diverticulae can be defined as herniations of the bladder mucosa through areas of weakness within the detrusor muscle. As they are only lined by a mucosal layer, both therapeutic and prognostic difficulties are encountered. They can be classified into congenital and acquired. The latter occurs as a result of increased intravesical pressure secondary to bladder outflow obstruction. These are common, usually multiple and are associated with a trabecular bladder. Unlike acquired diverticulae, congenital diverticulae are a result of disarray of the muscle fibres within the musculature of the bladder wall. They are rare, usually solitary and associated with vesico-ureteric reflux and hydronephrosis.1,2In addition, bladder diverticulae can usually occur in close proximity to the ureteric orifices.1
What is the most common neoplasm in the bladder diverticulae?
Transitional cell carcinomas (TCC) of a bladder diverticulum are rare and behave like bladder TCC elsewhere.1–3They are the most common primary neoplasm in the bladder diverticulae and are more prevalent in men. The incidence of TCC varies from 0.8% to 13%.4Due to the lack a muscular layer, stasis within the diverticulum increases the risk of development urological disease, including malignancy. Other risks are those associated with development of TCC elsewhere in the bladder. We report a TCC in a bladder diverticulum.
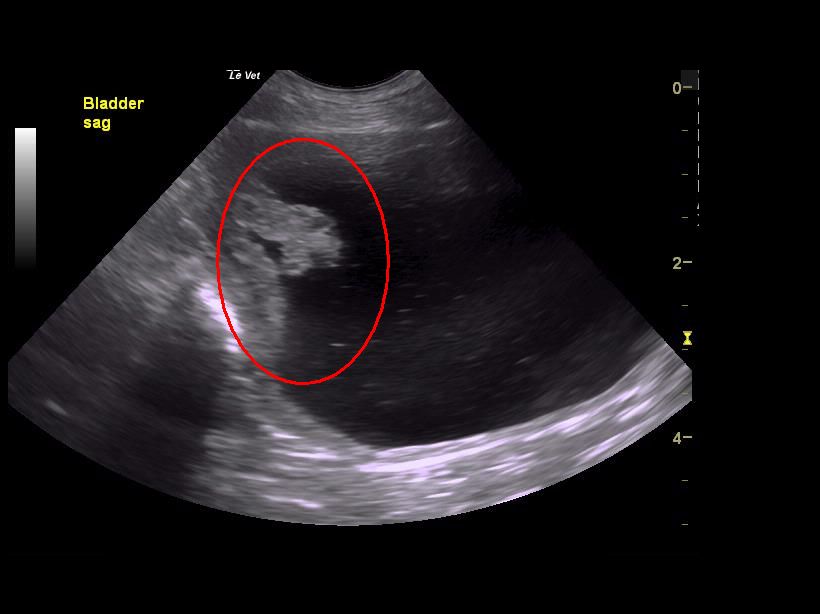
What is the fluid filled structure on the right posterior wall of the bladder?
Computed tomography (CT) showed a fluid filled structure on the right posterior wall of the bladder consistent with a bladder diverticulum. A bladder mucosal lesion consistent with TCC of the bladder was also identified within the bladder diverticulum. Magnetic resonance imaging (MRI) was subsequently performed to further characterize the anatomy of the lesion; it confirmed the finding of bladder tumour within bladder diverticulum arising from the right posterior wall of the bladder (Fig. 1a, Fig. 1b).
How many bladder tumors are non-muscle invasive?
Epidemiological studies have shown that 75% to 80% of bladder tumours present as non-muscle invasive, 70% of which are Ta lesions, 20% T1 lesions and 10% is Tis. The remaining 20% to 25% present as muscle invasive.12–14
Signs and Symptoms
- Symptoms of TCC will vary by the location of a tumor. They often resemble symptoms of a severe kidney infection wherein a person will experience painful urination and lower back/kidney pain. Because the disease mimics so many other possible causes (including cystitis, prostate infectio…
Causes and Risk Factors
- People will often assume that cancer of the bladderor kidneys is caused by exposure to toxins we ingest, whether it be contaminated water or chemicals in our food. For the most part, this is not the case. While toxins are definitely linked to the development of TCC, they are most often the types we inhale over long periods of time. Chief among these is cigarette smoke. In fact, over ha…
Diagnosis
- Generally speaking, the first diagnostic indication of TCC will be blood in urine. Sometimes it will not be visible but can be easily detected in a urinalysis (urine test). A urine cytology can also be used to look for cancer cells in urine, although this is a less reliable form of diagnosis. By contrast, newer technologies can identify proteins and other substances in urine associated with TCC. Th…
Cancer Staging
- If a cancer diagnosis is made, the oncologist will classify the malignancy by stage. The doctor will do so using the TNM staging system which describes the size of the original tumor ("T"), the infiltration of cancer into nearby lymph nodes ("N"), and the extent of metastasis("M"). The aim of the classification is to determine the appropriate course of action with aim of neither undertreati…
Drug Therapies
- Traditional chemotherapy drugs such as methotrexate, vinblastine, doxorubicin, and cisplatin are commonly used in combination therapy. They are cytotoxic (meaning toxic to living cells) and work by targeting fast-replicating cells like cancer. As a result of this action, they can also kill healthy cells that are fast-replicating such those in bone marrow, hair, and the small intestines. …
Prevention
- Prevention of TCC starts with the factors you can control. Of these, cigarettes remain the key focus. The facts are simple: bladder cancer is today the second most common smoking-related malignancy behind lung cancer. Quitting not only significantly reduces a person’s risk of TCC but can prevent cancer recurrence in those successfully treated. Quitting can be difficult and often r…