Byrdie.com
1. Organic Apple Cider Vinegar...
2. Fennel Seeds...
3. Aloe Vera...
4. Kudzu...
5. Apples, Bananas, Papaya...
6. Ginger...
7. Peppermint...
Learn More...Webmd.com
1. Angelica...
2. Caraway...
3. Clown's mustard plant...
4. German chamomile...
5. Greater celandine...
6. Lemon balm...
7. Licorice...
8. Milk thistle...
Learn More...Healthline.com
1. Aim for a healthy weight...
2. Know what foods and drinks to avoid...
3. Eat a little, sit up a little longer...
4. Eat foods that help...
5. Quit smoking...
6. Explore potential herbal remedies...
7. Avoid tight clothing...
Learn More...Allremedies.com
1. Baking Soda...
2. Aloe Vera Juice...
3. Chew Gum...
4. Do Not Lie Down...
5.Apple Cider Vinegar...
6. Know What Foods You Should Eat, How And When To Eat...
7. Eat An Apple Or A Banana...
Learn More...Fishertitus.org
1. Baking Soda...
2. Chew Gum...
3. Don't Lie Down After Eating...
4. Eat Fruit...
5. Ginger Tea...
6. Mustard...
7. Chamomile Tea...
Learn More...What is the best treatment of Gerd?
Treatment Approaches for GERD
- GERD Treatment: Lifestyle and Dietary Changes. Dietary and lifestyle changes are the first step in treating GERD. ...
- GERD Treatment: Medication. If lifestyle and dietary changes do not work, your doctor may prescribe certain medications. ...
- TIF and Other Endoscopic Therapy. ...
- Surgery for GERD
How to manage refractory Gerd?
- surgical treatment — specifically, laparoscopic Nissen fundoplication;
- active medical treatment, including omeprazole plus baclofen, with desipramine added depending on the patients’ symptoms; or
- control medication treatment, including omeprazole plus placebo.
What is the cure for the refractory?
Vaxiion Therapeutics to Initiate Phase 1 Clinical Trial of VAX014 for the Treatment of Solid Tumors Refractory to Standard Treatment Options SAN DIEGO--(BUSINESS WIRE)--Vaxiion Therapeutics, the industry leader in bacterial-minicell based cancer ...
Can GERD be cured or only treated?
Physiologic GERD (infrequent, related to meals) generally can be controlled or cured. But “clinically significant GERD” is only treatable Not curable in most cases. Clinically significant GERD (frequent, nocturnal, or complicated GERD) is usually not cured by diet or lifestyle modification alone.
What causes refractory GERD?
The causes of PPI-refractory GERD are numerous and diverse, and include adherence, persistent acid, functional disorders, nonacid reflux, and PPI bioavailability. The evaluation should start with a symptom assessment and may progress to imaging, endoscopy, and monitoring of esophageal pH, impedance, and bilirubin.
What is the last treatment for GERD?
PPIs are better at treating GERD symptoms than H2 blockers, and they can heal the esophageal lining in most people with GERD. You can buy PPIs over the counter, or your doctor can prescribe one. Doctors may prescribe PPIs for long-term GERD treatment.
What is the gold standard treatment for GERD?
PPIs: The most potent acid suppressive agents available are PPIs, and they tend to be the standard of care for patients with GERD.
What is the strongest medication for GERD?
PPIs are the most powerful medications available for treating GERD. These agents should be used only when this condition has been objectively documented. They have few adverse effects. However, data have shown that PPIs can interfere with calcium homeostasis and aggravate cardiac conduction defects.
Are there any new treatments for GERD?
The newest therapy is the transoral incisionless fundoplication (TIF). This is an incisionless fundoplication performed with an endoscope that is inserted through the mouth and into the stomach. Short-term results appear favorable in carefully selected patients; however, long-term studies have not yet been completed.
What is the first line of treatment for GERD?
Mild symptoms — In addition to lifestyle changes, the initial treatment of mild GERD includes the use of nonprescription antacids or histamine receptor antagonists. Antacids/alginates — Antacids (sample brand names: Tums, Maalox) neutralize stomach acid and are commonly used for short-term relief of heartburn symptoms.
What is the first line medication for GERD?
H2 receptor antagonists and H2 blocker therapy H2 receptor antagonists are the first-line agents for patients with mild to moderate symptoms and grades I-II esophagitis. Options include cimetidine (Tagamet), famotidine (Pepcid), and nizatidine (Axid).
Which is better TIF or Linx?
The LINX procedure and the TIF EsophyX procedure both have a very low incidence of bloating side effects. The LINX procedure does have more issues with swallowing problems (food sticking) than the EsophyX, but it may have greater success at controlling GERD symptoms long-term than TIF/EsophyX.
What is weakly acidic reflux?
Weakly Acidic or Nonacid Reflux Two multivariate analyses posited that reflux episodes that extend proximally with mixed liquid-gas composition are significantly associated with symptoms regardless of pH status of the reflux. 36,37 Weakly acidic reflux is defined as any reflux event in which the esophageal pH falls by 1 unit or more but is still less than 4 as measured by pH impedance. 38 The mechanism by which weakly acidic or nonacid reflux may cause symptoms is not completely understood, but is thought to be a combination of mechanical distention and/or reflux contents. Two studies implicated mechanical distention by replicating heartburn symptoms with mechanical balloon dilation with esophagogastroduodenoscopy (EGD) in patients. 39,40 Additionally, both bile acid and pepsin may be present in weakly acidic or nonacid reflux and may contribute to chemical irritation of the esophageal lining. 41,42 Previous acid exposure likely leads to esophageal pain and hypersensitivity when exposed to weakly acidic or nonacid reflux contents regardless of pH. 43 Future studies are warranted to further clarify the relationship between refractory GERD and weakly acidic and nonacid reflux.
What is the fax number for GERD?
Fax: 615-322-8525. E-mail: [email protected]. Download PDF. Abstract: Gastroesophageal reflux disease (GERD) is a common disorder that is treated with lifestyle modification, weight loss, and medications, such as proton pump inhibitors (PPIs). An empiric course of PPI therapy is an effective and cost-effective strategy for the management ...
What is the name of the reflux of the duodenal contents through the stomach and into the eso?
Duodenogastroesophageal Reflux Duodenogastroesophageal reflux (DGER) refers to the reflux of duodenal contents through the stomach and into the esophagus. Bile acids may play a role in refractory GERD through either weakly acidic or nonacid reflux.
What is the term for a delay in gastric emptying?
Gastroparesis Gastroparesis is characterized by a delay of gastric emptying into the small intestine leading to increased reflux. Symptoms typically include epigastric pain, early satiety, postprandial bloating, and nausea. 22 There has been a small, established association between refractory GERD and gastroparesis, with 1 study revealing that refractory GERD patients with erosive esophagitis were more likely to have delayed gastric emptying compared to patients with erosive esophagitis but no symptoms. 65
Does PPI cause acid reflux?
An acid pocket may migrate into the esophagus shortly after eating, causing potential reflux symptoms. PPI use can reduce the size of this pocket and increase gastric pH. 53 However, it is not known how significantly, if at all, the acid pocket contributes to refractory GERD.
Can GERD be missed?
Missed Gastroesophageal Reflux Disease Current testing for GERD has limitations and can lead to a missed diagnosis. Catheter-based testing can be uncomfortable and can limit typical eating patterns in patients, thus leading to uncharacteristic acid reflux patterns and increasing the potential for false-negative results. 47-49 Although ambulatory pH monitoring has been shown to decrease patient discomfort, false-negative results have been reported up to 30% of the time. 50 GERD is a chronic condition; therefore, measuring pH events over a 48-hour period likely fails to capture the chronic nature of this disease. 51,52 Research has yet to elucidate the role of missed gastroesophageal reflux in symptomatic refractory GERD, but ongoing studies are better understanding the role of esophageal mucosal integrity testing as a more beneficial surrogate for GERD. 52
Is GERD a PPI?
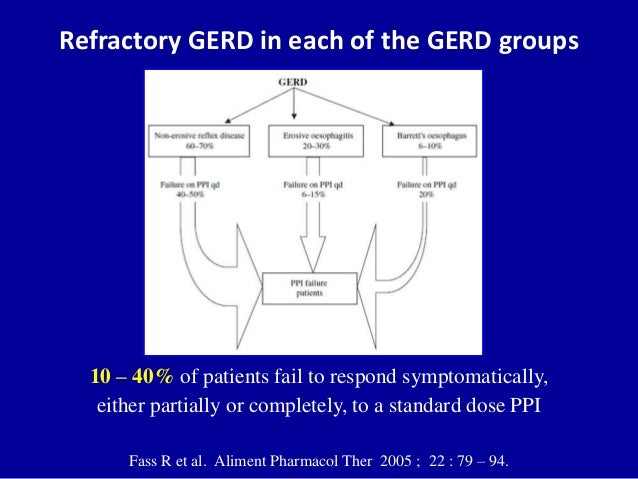
GERD can be subdivided into erosive reflux disease or nonerosive reflux disease (NERD) based on endoscopic findings. Both types exhibit variable success with PPI therapy. Patients with NERD do not have findings of esophagitis on endoscopy but do have typical symptoms of GERD, with generally high esophageal acid exposure time on pH monitoring. In one study, patients with NERD, who make up to 70% of the GERD population, had a lower effective response rate to once-daily PPI therapy at 4 weeks compared to patients with erosive esophagitis (37% vs 56%, respectively), with a similar study showing comparable results. 12,14 Patients who have a normal acid exposure time but a positive symptom index (SI) or symptom association probability (SAP) are classified as having reflux hypersensitivity. If heartburn remains the predominant symptom but the SI and SAP are normal, patients are classified as having functional heartburn according to the Rome IV criteria. 15 Both of these functional esophageal disorders are the etiology of persistent symptoms in refractory GERD in up to 90% of patients. 16 There is often concomitant typical GERD with these 2 functional esophageal disorders. According to one study, in 75% of patients with GERD refractory to once-daily PPI therapy, 62.5% had functional heartburn and 12.5% had reflux hypersensitivity. 17 Given this predominance of functional esophageal disease overlap, treatments should be aimed at neuromodulation, psychological therapy, and complementary therapy as opposed to increased antireflux medications or surgical or endoscopic interventions. 18
What is rgerd symptomatic?
Background Refractory gastroesophageal reflux disease (rGERD) can be characterized as symptomatic reflux or esophagitis despite an adequate trial of twice daily proton pump inhibitor (PPI) therapy (1). Patients with rGERD might describe their symptoms as heartburn, poorly localized chest pain, or acid reflux. Non-verbal patients (e.g. patients obtunded from the dying process) may be at risk of untreated GERD. This Fast Fact reviews treatment options for rGERD in patients with life-limiting illness.
What are the mechanisms of rgerd?
Etiologies Mechanisms that contribute to rGERD in palliative care populations are varied and include both gastrointestinal and non-gastrointestinal processes such as: increased esophageal acid exposure (i.e. secondary to gastric carcinoid tumors); opioid-induced gastroparesis/delayed emptying; and/or peristaltic deficiency associated with cirrhotic ascites; malignancy-induced bowel obstructions; and transient lower esophageal sphincter relaxation (TLESR) (1,2). Clinicians should consider rGERD in the differential diagnosis of non-verbal patients who appear to be imminently dying and are uncomfortable, especially if they have a history of GERD, cancer, and/or cirrhosis.
Is metoclopramide good for rgerd?
Metoclopramide is a prokinetic agent that may improve rGERD symptoms and nausea in patients with delayed esophageal peristalsis, delayed gastric emptying (gastroparesis), and partial bowel obstruction at oral or parenteral doses of 10 mg three to four times a day. It is not recommended nor effective for patients who do not have evidence of gastroparesis or a partial bowel obstruction (9). It has been associated with adverse effects such as tardive dyskinesia and dystonia, especially if used for longer than 12 weeks (9).
Does ranitidine help with reflux?
Adding a nocturnal histamine-2 receptor antagonist (H2RA) such as ranitidine for at least one month while on concurrent PPI therapy has been associated with improvements in night-time reflux symptoms, GERD-associated sleep disturbance, and overall GERD symptom management in up to 74% of patients; only 13% discontinued nocturnal H 2 RA due to tolerance issues (3). Coadministration of H 2 RAs and PPIs is felt to be safe (4), although some experts suggest separating evening PPI and bedtime H 2 RA doses for optimal effect. Solutions containing sodium alginate (i.e. Gaviscon®) have reliably decreased the severity and frequency of heartburn, especially when used post-prandially, with few side effects (5,6). Likewise, sucralfate in two-to-four daily doses may improve rGERD as well as mucosal healing for erosive disease (7). However, none of these agents have been well-studied in the seriously ill.
Does smoking reduce esophageal sphincter pressure?
Lifestyle interventions: Although, tobacco use, and alcohol consumption may reduce lower esophageal sphincter pressure, cessation of these agents has not been clearly shown to lead to improvements in GERD symptoms (13). Some experts recommend head of bed elevation and avoidance of a late-night evening meal (within 2-3 hours of bedtime) to mitigate rGERD, although the degree to which these interventions help is not clearly established (14).
Is rgerd a symptom management?
Symptom Management When possible, therapeutic management of rGERD should target the underlying etiology (e.g. triple therapy for helicobacter pylori). However, in palliative care patients, clinicians must factor in prognosis, the amount of symptom distress, and the clinical situation to determine the extent of diagnostic work-up (e.g. endoscopy) and specialized consultation that is appropriate. For many palliative care patients, empiric treatment of rGERD is pursued.
Does trazodone help with GERD?
Antidepressants Selective serotonin reuptake inhibitors and trazodone have been shown to reduce GERD symptoms in symptomatic patients with normal endoscopies (10-12). Citalopram and fluoxetine have both been shown to be effective in placebo-controlled randomized trials (10,11) and even showed superiority to omeprazole in controlling heartburn symptoms in one comparison trial in patients with concomitant depression (11). Evidence for trazodone has been limited to the symptomatic relief of chest pain in patients with esophageal contraction abnormalities (12).
What is refractory GERD?
The paper’s authors defined refractory GERD as “persisting objective GERD evidence despite medical therapy (erosive esophagitis, or abnormal esophageal acid exposure and/or elevated numbers of reflux episodes on reflux monitoring performed on therapy).”
How long does it take for GERD to respond to proton pump inhibitor?
Refractory GERD symptoms are partially responsive or nonresponsive to a stable dose of a proton pump inhibitor (PPI) during treatment of at least 8 weeks in patients with prior objective evidence of GERD, according to the consensus paper’s authors.
Can esophageal motility be assessed?
The guideline recommended that esophageal motility should be assessed using high-resolution manometry in patients with refractory GERD symptoms. High-resolution manometry can rule out major esophageal motility disorders and demonstrate esophagogastric junction and esophageal body motor abnormalities associated with GERD, noted the paper’s authors. In asymptomatic patients with untreated Barrett esophagus, testing for persisting reflux in the setting of PPI therapy is not recommended, according to the paper.
Is grade B/C/D esophagitis refractory?
According to the position paper, Los Angeles grade B/C/D esophagitis on endoscopy despite optimized PPI therapy is indicative of refractory GERD. In patients who have refractory GERD symptoms, nonspecific inflammation on esophageal biopsy specimens is not relevant, and the diagnostic yield of eosinophilic esophagitis is very low in the absence of dysphagia and specific endoscopic signs. In addition, Barrett mucosa of any length does not indicate poor GERD control, noted the authors.
Can GERD be related to PPI?
In patients with proven GERD and a large hiatal hernia, persistent regurgitation on PPI therapy is likely to be related to refractory GERD, according to the paper.
Does antireflux surgery help with GERD?
The position paper recommended that antireflux surgery, including laparoscopic fundoplication and magnetic sphincter augmentation, improves refractory GERD symptoms, particularly regurgitation, in patients with proven GERD. Some research has shown that laparoscopic fundoplication is comparable to long-term PPI therapy in well-characterized GERD.
Does Barrett mucosa indicate GERD?
In addition, Barrett mucosa of any length does not indicate poor GERD control, noted the authors. “Endoscopic and/or radiologic evaluation of esophagogastric junction morphology should be performed in patients with refractory GERD symptoms,” advised the authors. The position paper recommends that patients with persistent esophageal ...
What is the treatment for GERD?
Treatment for GERD includes: Lifestyle and dietary changes. Medication. Endoscopic therapy. Surgery.
How to treat GERD?
Dietary and lifestyle changes are the first step in treating GERD. Certain foods make the reflux worse. Suggestions to help alleviate symptoms include: 1 Lose weight if you are overweight — of all of the lifestyle changes you can make, this one is the most effective. 2 Avoid foods that increase the level of acid in your stomach, including caffeinated beverages. 3 Avoid foods that decrease the pressure in the lower esophagus, such as fatty foods, alcohol and peppermint. 4 Avoid foods that affect peristalsis (the muscle movements in your digestive tract), such as coffee, alcohol and acidic liquids. 5 Avoid foods that slow gastric emptying, including fatty foods. 6 Avoid large meals. 7 Quit smoking. 8 Do not lie down immediately after a meal. 9 Elevate the level of your head when you lie down.
What is a TIF for GERD?
Transoral incisionless fundo plication (TIF) is an option to address GERD. TIF can mean a shorter treatment time, less pain and faster recovery compared to laparoscopic surgery. The procedure involves using a special TIF device to create a passageway for a flexible, tube-like imaging instrument called an endoscope. The procedure allows the physician to use preloaded tweezers and fasteners to repair or recreate the valve that serves as a natural barrier to reflux.#N#Currently, there are clinical trials testing the efficacy of endoscopic therapy for GERD. One form of therapy uses an endoscopic sewing machine to place sutures in the stomach and increase the anti-reflux barrier.
What is the purpose of surgery for reflux?
The goal of surgery for reflux disease is to strengthen the anti-reflux barrier. During a procedure known as a Nissen fundoplication, your surgeon wraps the upper part of your stomach around the lower esophagus. This enhances the anti-reflux barrier and can provide permanent relief from reflux.
How to help with reflux?
Suggestions to help alleviate symptoms include: Lose weight if you are overweight — of all of the lifestyle changes you can make, this one is the most effective. Avoid foods that increase the level of acid in your stomach, including caffeinated beverages.
What is the best medicine for reflux?
Antacids. Over-the-counter antacids are best for intermittent and relatively infrequent symptoms of reflux. When taken frequently, antacids may worsen the problem. They leave the stomach quickly, and your stomach actually increases acid production as a result.
Can you have surgery for GERD?
Surgery for GERD. If your symptoms did not improve with lifestyle changes or drug therapy, you may be a candidate for surgery. Some patients prefer a surgical approach as an alternative to a lifetime of taking medications. The goal of surgery for reflux disease is to strengthen the anti-reflux barrier.
What is refractory GERD?
The definition of “refractory GERD” has traditionally been described as a group of varying symptom presentations related to GERD, which persists even though the patients accepted the standard daily PPI therapy for at least 12 weeks.
How to monitor esophageal reflux?
There are two methods for esophageal reflux monitoring, called as On-PPI and Off-PPI. In off-PPI (7 days after cessation of PPI), the presence of abnormal acid reflux and/or positive symptom-reflux relationship can be confirmed. The relevant parameter to be observed is esophageal acid exposure, which is the proportion of time (in minutes or percentage of time) spent below pH 4, as well as correlation between symptoms and reflux events (symptom index (SI) and/or symptom association probability (SAP)). Positive symptom association with normal esophageal acid exposure is considered hypersensitive esophagus (HE), reflecting an underlying visceral hypersensitivity. For on-PPI reflux monitoring, impedance-pH monitoring should reasonably be proposed as the preferred investigation. It can detect nonacid reflux during the PPI therapy period, which is one of causes for persistent GERD symptom. It also can figure out whether acid reflux is controlled or not by the treatment ( Table 1 ).
What is the Stretta procedure?
Stretta procedure and EsophyX transoral incisionless fundoplication are two antireflux endoscopic devices which are clinically available . The Stretta procedure showed clinical improvement of esophageal symptoms and a decrease in PPI use but no significant effect on esophageal acid exposure [ 10 ]. EsophyX offers a less invasive alternative to laparoscopic fundoplication for PPI-dependent GERD patients, which still needs further studies to demonstrate its efficiency.
What are the symptoms of GERD?
The patients with GERD suffer from typical symptoms such as heartburn and regurgitation, as well as other atypical symptoms including chest pain, cough, asthma, and hoarseness.
Is antireflux surgery good for GERD?
Comparing with patients with adequate PPI symptom control, antireflux surgery might have a less favorable clinical outcome for the patients with refractory GERD symptom. Normal acid exposure and the presence of atypical reflux symptoms and persisting symptoms despite PPI therapy are predictors of a poor postoperative outcome. It is important to confirm pathological reflux before considering antireflux surgery if there is no proven esophagitis. Summarily, surgery can be a valuable option in patients with typical reflux symptoms with inadequate response to PPIs, provided abnormal esophageal acid exposure and/or positive symptom association analysis in off-PPI test [ 11 ].
Is GERD a refractory condition?
However, the treatment of GERD fails in a proportion of patients despite the high efficacy of PPIs. This situation is referred as to refractory GERD symptoms. What is worse, it is getting more and more common in clinical practices. In this chapter, we will discuss about this difficult situation, emphasizing on diagnosis and treatment, combined with suggested management of these patients.
Is anxiety a refractory disorder?
Psychological disorders such as hysteria, anxiety, and distress should also be evaluated in patients with refractory symptoms. Weak correlation of symptoms with acid reflux events might indicate a high level of anxiety and hysteria as compared with patients who demonstrate a close correlation between symptoms and acid reflux event [ 6 ]. Anxiety and depression have been shown to increase reflux symptoms reported in population-based studies. A study has reported that patients who did not respond to PPI treatment were suffered from more psychosocial problem [ 7 ].