Medication
Other common ailments for those with hyperglobulinemia can include:
- Diarrhea
- Fatigue
- Anemia
- Spleen, liver, lymph nodes, and tonsils enlargement
- Stiffness in joints, especially the hips and knees
Therapy
Instead, CVID that develops later in life is now referred to as adult-onset hypogammaglobulinemia. While there is currently no cure for CVID, treatment can help alleviate symptoms and prevent infections that are associated with the disease.
Self-care
Prognosis. Prognosis is often dictated by the underlying condition. Despite this, early detection and treatment of hypogammaglobulinemia does reduce morbidity rates and the chance of long-term pulmonary complications. [12]
Nutrition
Signs that a person may have an immune deficiency disorder:
- Recurrent, unusual, or difficult to treat infections
- Delayed growth and development
- Blood disorders, such as low platelet counts or anemia
- Recurrent pneumonia, ear infections or sinusitis
- Swollen lymph glands or an enlarged spleen
How do they treat hypogammaglobulinemia?
Is there a cure for hypogammaglobulinemia?
What is the prognosis of hypogammaglobulinemia?
What is Ig replacement therapy?
See more
Is hypogammaglobulinemia serious?
People with hypogammaglobulinemia can more easily catch pneumonia, meningitis, and other infections that a healthy immune system would normally protect against. These infections can damage organs and lead to potentially serious complications.
What does it mean to have hypogammaglobulinemia?
Hypogammaglobulinemia is a disorder caused by low serum immunoglobulin or antibody levels. Immunoglobulins are the main components of the humoral immune response and able to recognize antigens to trigger a biological response and eradicate the infectious source.
What medications can cause hypogammaglobulinemia?
Hypogammaglobulinemia may result from other anticonvulsants and anti-inflammatory medications, including valproic acid, phenytoin, gold, sulfasalazine, chloroquine, penicillamine, fenclofenac, hydantoin, zonisamide, lamotrigine, and cyclosporine A (1, 4, 5, 9).
How do you treat hypergammaglobulinemia?
Since hypergammaglobulinemia is caused by other conditions, there aren't many direct treatment options available. But you can improve or cure this condition by treating other underlying infections, immune disorders, and diseases. One uncommon treatment for this condition is immunoglobulin replacement therapy.
How do you get hypogammaglobulinemia?
The most common cause is common variable immunodeficiency (CVID). Causes of secondary hypogammaglobulinemia include gastrointestinal losses (e.g., malabsorption/protein-losing enteropathy), nephrotic syndrome, hematologic malignancy, and medication (e.g., immunosuppressives, such as corticosteroids and chemotherapy).
Can you grow out of hypogammaglobulinemia?
Most children born with transient hypogammaglobulinemia of infancy will grow out of it between the ages of 2 and 5. Other types of hypogammaglobulinemia are lifelong conditions. The risk of infection can be reduced by different treatments, depending on the type and cause of hypogammaglobulinemia.
What kind of doctor treats IgG deficiency?
You'll likely start by seeing your family doctor or primary doctor. You might then be referred to a doctor who specializes in disorders of the immune system (immunologist).
How do you diagnose hypogammaglobulinemia?
DiagnosisSerum immunoglobulin levels (IgA, IgG, and IgM)Complete blood count with differential.Antibody response for recall antigens.Isohemagglutinins (especially useful if patient already received IV or SC Ig)Peripheral blood lymphocyte immunophenotyping.More items...•
Is hypogammaglobulinemia considered a disability?
Hypogammaglobulinemia does not have a specific heading under the Social Security Administration's Listing of Impairments.
When do you give IVIG for hypogammaglobulinemia?
4) Dose - IVIG is indicated for patients with primary immunodeficiency at a starting dose of 400- 600 mg/kg every 3-4 weeks. Less frequent treatment, or use of lower doses, is not substantiated by clinical data.
Is hypogammaglobulinemia genetic?
The identification of genes and pathways involved in hypogammaglobulinemia has generated considerable interest. Defects in many of the genes that cause immunodeficiency result in a phenotype that is different from that seen in mice with mutations in the same genes [31,40].
What is secondary hypogammaglobulinemia?
Secondary hypogammaglobulinemia (SHG) is characterized by reduced immunoglobulin levels due to a medication or a disease process, leading to decreased antibody production or increased antibody loss.
What causes hypogammaglobulinemia?
Causes of secondary hypogammaglobulinemia include gastrointestinal losses (e.g., malabsorption/protein-losing enteropathy), nephrotic syndrome, hematologic malignancy, and medication (e.g., immunosuppressives, such as corticosteroids and chemotherapy). Patients can be predisposed to recurrent upper and lower respiratory tract infections.
Is hypogammaglobulinemia a primary or secondary condition?
Summary. Hypogammaglobulinemia can be primary (congenital) or secondary. It can present in childhood and in adults, and can affect both sexes. Primary hypogammaglobulinemia (most common cause being common variable immunodeficiency [CVID]) may have a delay of several years between clinical presentation and diagnosis.
Why is hypogammaglobulinemia rare?
Hypogammaglobulinemia may be due to certain genetic diseases or to acquired diseases such as HIV. Most patients with hypogammaglobulinemia present with a history of recurrent infections, failure to thrive, autoimmune disease, and more rarely with malignancies (especially leukemias or lymphomas).
When does IgG disappear?
Found in male babies expressed around 5 to 6 months of age (maternal IgG disappears)
Is transient hypogammaglobulinemia an inherited disorder?
Onset during early childhood suggests an inherited disorder. However, the condition transient hypogammaglobulinemia of infancy, as its name implies, represents a delay in the maturation of the full range of antibody responses, and usually resolves by a few years of age.
Is IgA more common than other deficiencies of immunoglobulins?
IgA deficiency is more common than other deficiencies of immunoglobulins 6).
What are the causes of hypogammaglobulinemia?
Humoral immunological defects are frequent and important causes of hypogammaglobulinemia, leading to recurrent infections, autoimmunity, allergies, and neoplasias. Usually, its onset occurs in childhood or during the second and third decades of life; however, the diagnosis is made, on average, 6 to 7 years afterwards. As a consequence, antibody defects can lead to sequelae. Here we describe the clinical-laboratory characteristics, treatment, and prognoses of patients with hypogammaglobulinemia. An observational, cross-sectional, and retrospective study of patients attending the recently established outpatient group of Clinical Immunology between 2013 and 2018 was carried out. Patients with IgG levels below 2 standard deviations from the mean values for the age and/or impaired antibody response were included. Eight patients (3 F and 5 M; median age=41 years (16–65), average symptom onset at 25 years (1–59), and time to diagnosis of 10 years were included. The main infections were: sinusitis in 7/8, pneumonia in 6/8, otitis in 2/8, tonsillitis and diarrhea in 2/8, and diarrhea in 2/8 patients. Hypothyroidism was identified in 4/8 (50%) patients. Rhinitis was found in 7/8 (87.5%) and asthma in 3/8 (37.5%) patients. The tomographic findings were consolidations, atelectasis, emphysema, ground glass opacity, budding tree, bronchial thickening, and bronchiectasis. Immunoglobulin reposition was used between 466 and 600 mg/kg monthly (514.3 mg·kg-1·dose-1). Prophylactic antibiotic therapy was included in 7/8 (87.5%) patients. Airway manifestations prevailed in patients with hypogammaglobulinemia. There is a need for educational work to reduce the time of diagnosis and initiation of treatment, avoiding sequelae.
Where was the hypogammaglobulinemia study carried out?
An observational, cross-sectional, and retrospective study was carried out at the Outpatient Clinic of Clinical Immunology at ABC University Health Center , which analyzed the medical records of patients with hypogammaglobulinemia between 2013 and 2018. The study was approved by the Research Ethics Committee of the ABC Medical School (CAAE 34466214.9.0000.0082), and written informed consent was obtained from all participants and/or guardians.
How is immunoglobulin replacement administered?
The treatment can be administered intravenously or subcutaneously with variable doses, as determined by an individualized orientation. The dose prescribed by the investigators ranged from 466 to 600 mg/kg per month, with good clinical response and serum IgG levels in 5 patients. The route of administration had to be changed from intravenous to subcutaneous in one patient due to adverse effects and in another patient due to the need for a higher dosage to reach adequate levels. After the review of immunoglobulin concentrations, patient 1 stopped receiving immunoglobulin replacement as previously described.
What is the mortality rate of granulomatous lymphocytic interstitial lung disease?
An interstitial lung disease known as granulomatous lymphocytic interstitial lung disease (GLILD) is often found and has a higher mortality rate, occurring in at least 10–20% of patients with CVI. GLILD presents tomographic findings distinct from the usual airway abnormalities commonly associated with CVI: pulmonary micronodules, thoracic lymphadenopathy, interlobular septal thickening, and multifocal pulmonary consolidation (21). Although atelectasis (3), bronchiectasis (2), ground glass opacity (4), and budding tree (2) were found, the criteria for granulomatosis diagnosis were not met by our patients.
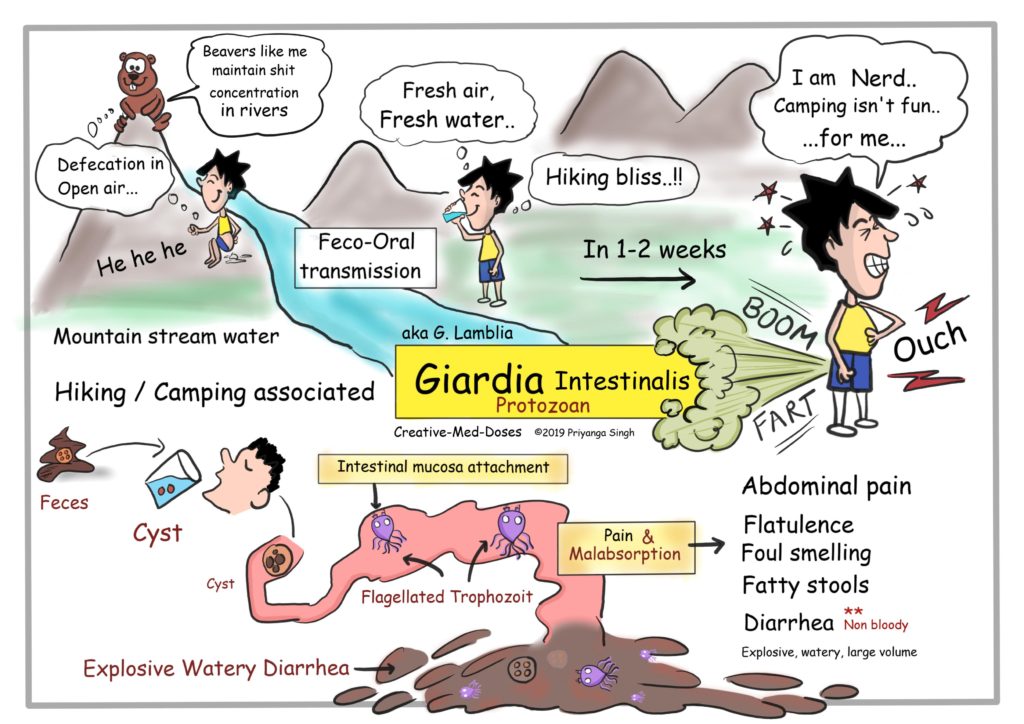
What are the most common clinical manifestations of Sinopulmonary infections?
Sinopulmonary infections (pneumonia, bronchitis, sinusitis, otitis, and conjunctivitis) by encapsulated bacteria and gastrointestinal infections (Giardia lambliadiarrhea) are the most common clinical manifestations (13,14). Although bacterial infections are characteristic of humoral immunity defects, Sperlich et al. (15) identified viral infection in 30 (56%) of 54 nasopharyngeal swabs collected in 41 immunodeficient patients. Rhinoviruses were most commonly detected (33%), but one of the patients presented metapneumovirus infection similar to one of the patients in our outpatient clinic (15).
Is hypogammaglobulinemia a disease?
Hypogammaglobulinemias are heterogeneous diseases of either primary origin (genetic disorders and/or chromosome anomalies) or secondary origin (induced by extrinsic factors – infectious agents, mediators such as corticosteroids and immunosuppressants, chemotherapy, metabolic diseases such as nephrotic syndrome, nutritional disorders, and environmental conditions such as ionizing radiation) (4). Among the conditions associated with hypogammaglobulinemia, common variable immunodeficiency (CVI) is the most common disorder associated with antibody deficiency and has a notably high prevalence, affecting one in every 10,000–50,000 live births.
Is hypogammaglobulinemia a primary immunodeficiency?
Hypogammaglobulinemia may occur due to multiple causes. Of the primary immunodeficiencies, CVI is the most prevalent after IgA deficiency (1:1000 individuals) (11). In Brazil, a prevalence rate of 1:66,000–75,000 has been estimated (11). These data exhibit significant variability in several countries, likely due to healthcare accessibility, time to diagnosis, or even lack of patient identification. The genetic differences among the populations may also be relevant (4).
What is a X-linked agammaglobulinemia?
Both the X-linked (Bruton agammaglobulinemia), accounting for 85% of cases, and autosomal recessive forms are associated with extremely low number or absence of B cells. Agammaglobulinemia is characterized by serum IgG levels of less than 100 mg/dl, IgM of less than 20 mg/dl, IgA of less than 10 mg/dl, and peripheral CD-19+ B cell of less than 2%. The principal manifestation is recurrent upper and lower respiratory tract infections. A continual IgRT is an absolute necessity and is life saving. Retrospective analyses of data from agammaglobulinemic children have revealed that the number and severity of infectious complications are inversely correlated with the dose of IVIG administered. Serious bacterial infections and enteroviral meningoencephalitis were prevented when the IgG trough levels were maintained above 800 mg/dl.
When is immunoglobulin replacement necessary?
In SCID, immunoglobulin replacement is also necessary in the post-transplantation period, during gene therapy or enzyme replacement (for adenosine deaminase deficiency), until B-cell function is restored.
What is IgRT therapy?
The goals of immunoglobulin (Ig) replacement therapy (IgRT) for patients with primary immunodeficiency is to provide adequate replacement immunoglobulins to minimize potentially fatal infections and prevent complications associated with the disease and improve quality of life. A brief overview of benefits of IgRT is in some of the phenotype ...
What are the three categories of immunoglobulin?
The disorders for which immunoglobulin is variably used fall into three categories: (1) Milder forms of combined immunodeficiencies (such as that caused by partially functional mutations in recombinase-activating genes [RAG]) and (2) Combined immunodeficiencies with associated or syndromic features (such as Wiskott-Aldrich syndrome).
Can IgRT be used for CLL?
However, the FDA has approved use of IgRT in patients with chronic lymphocytic lymphoma (CLL) and recurrent serious bacterial infections, low IgG levels, and sub protective antibody levels after vaccination. Numerous studies have shown the benefit of decreasing documented infections but without survival benefits.
Can IgG be used for chylothorax?
Secondary hypogammaglobulinemia due to increased IgG loss can occur in may conditions (as discussed earlier) including chylothorax, lymphaniectasia, or protein-losing enteropathy or medications like anti seizure, corticosteroids or rituximab do not warrant IgG administration. However, the FDA has approved use of IgRT in patients with chronic lymphocytic lymphoma (CLL) and recurrent serious bacterial infections, low IgG levels, and sub protective antibody levels after vaccination. Numerous studies have shown the benefit of decreasing documented infections but without survival benefits.
Is IgG administration considered a failure?
Antibiotics both for treatment and prophylaxis is the initial step and IgG administration is only considered with antibiotic failure or significant recurrent infections . Continued close monitoring for recovery and excluding other causes of hypogammaglobulinemia is important.
How to treat hypogammaglobulinemia?
Hypogammaglobulinemia is often controlled through the use of IVIG (Intravenous Gamma globulin). This should be administered after 21 or 28 days subcutaneously or intravenously.
What is the diagnosis of hypogammaglobulinemia?
Hypogammaglobulinemia diagnosis. Diagnosis of hypogammaglobulinemia starts with a physical test and evaluation of the patient’s family medical history. Normally, the physical assessment is standard for individuals having agammaglobulinemia. Examination is an important aspect of the diagnosis of hypogammaglobulinemia.
What is secondary control of hypogammaglobulinemia?
Important information. Hypogammaglobulinemia is a medical complication brought about by a deficiency of B-cells (B-lymphocytes) in addition to a resultant decrease in the amount of antibodies (immunoglobulin) in the body system. These antibodies play a twofold part in the body’s immune system by allowing ...
What should be considered before starting hypogammaglobulinemia treatment?
Before the start of hypogammaglobulinemia treatment, the health care provider should consider the dangers and advantages of administering any medications that can reduce the level of antibodies in the patient’s bloodstream.
Is hypogammaglobulinemia a pitiable disease?
Results are pitiable in case hypogammaglobulinemia is not discovered and treated, especially in cases of a bronchiectasis or a severe destruction of the lungs. Sadly, the diagnosis ends up being overly late, thereby increasing the risks for a number of pulmonary infections and this attributes to reduced life expectancy of hypogammaglobulinemia.
Does hypogammaglobulinemia reduce morbidity?
However, early diagnosis and treatment for hypogammaglobulinemia may not help to minimize the rates of morbidity as well as the risks for lasting pulmonary infections. Proof indicates that there is a relationship between large amounts of IgG and decreased frequency of infections.
Is hypogammaglobulinemia a prognosis?
Hypogammaglobulinemia prognosis. It is generally hard to oversimplify the prognosis of hypogammaglobulinemia because possibly there are a number of other underlying complications. This takes into account the fact that hypogammaglobulinemia prognosis is determined by the results of all underlying complications.
What is hypogammaglobulinemia?
Hypogammaglobulinemia is an immune disorder characterized by a reduction in all types of gamma globulins, including antibodies that help fight infection. It may be congenital (present at birth), related to medication; it may be due to a kidney or gastrointestinal condition, cancer or severe burns.
Common symptoms reported by people with hypogammaglobulinemia
Reports may be affected by other conditions and/or medication side effects. We ask about general symptoms (anxious mood, depressed mood, fatigue, pain, and stress) regardless of condition.
Treatments taken by people for hypogammaglobulinemia
Data from patients with hypogammaglobulinemia, who have ever reported treatments, ordered by their reporting frequency during the last 5 years.
Compare treatments taken by people with hypogammaglobulinemia
Data from patients with hypogammaglobulinemia, who have ever reported treatments, ordered by their reporting frequency during the last 5 years.
How to diagnose hypogammaglobulinemia?
Diagnosis of hypogammaglobulinemia starts with a physical test and evaluation of the patient’s family medical history. Normally, the physical assessment is standard for individuals having agammaglobulinemia.
What is the debilitating effect of hypogammaglobulinemia?
Hypogammaglobulinemia, also known as Common Variable Immunodeficiency (CVID), is a disorder that falls into the category of the primary immunodeficiency diseases, meaning its main debilitating effect on the body is a weakening of the immune system that makes the individual susceptible to higher rates of infection and illness, among other symptoms.
What tests are performed to diagnose hypogammaglobulinemia?
Some of the tests that are carried out during the assessment of agammaglobulinemia are serum IgM test, serum IgA test, and serum IgG test and serum immunoelectrophoresis.
What is the name of the disorder where the body makes low amounts of infection-fighting antibodies?
Hypogammaglobulinemia is a disorder in which the body makes low amounts of infection-fighting antibodies (also known as gamma globulins). This leaves the person susceptible to infections. About 5% to 10% of thymoma patients develop hypogammaglobulinemia. About 10% of patients with hypogammaglobulinemia have a thymoma.
What is the medical term for elevated gamma globulin?
Hypogammaglobulinemia is a medical condition with elevated levels of gamma globulin. It is a type of immunoproliferative disorder. Hypogammaglobulinemia is an immune disorder characterized by a reduction in all types of gamma globulins, including antibodies that help fight infection.
How does prognosis affect IVIG?
Prognosis has improved significantly since the introduction of IVIG therapy to routine practice. The prognosis largely depends on whether there is severe autoimmune disease; whether there are recurrent infections that cause structural lung damage; and the development of a malignancy (cancer). Other major factors that influence prognosis include the extent of end-organ damage and how successfully infections can be prevented.
Can a negative family history exclude X-linked agammaglobulinemia?
A positive family history may suggest the diagnosis and guide testing, but a negative family history does not exclude X-linked agammaglobulinemia (Bruton agammaglobulinemia; XLA), as new mutations may constitute more than half of the cases in some series. Duloxetine, Sertraline and Paroxetine can be used as medications.