Treatment for gastrointestinal infection includes taking antibiotics and staying hydrated. Common antibiotics used to treat gastrointestinal infection are penicillin, cephalosporin, antifolate / sulfa combinations, nitroimidazole, penem, glycopeptide, and monobactam antibiotics.
Full Answer
What kind of medications are used in gastroenterology?
Nizatidine to reduce stomach acid. Olsalazine for ulcerative colitis. Omeprazole to reduce stomach acid (Losec, Mepradec, Prilosec) Orlistat capsules (Alli, Beacita, Orlos, Xenical) Pancreatin (Creon, Nutrizym, Pancrease, Pancrex) Pantoprazole to reduce stomach acid.
What is the role of the gastrointestinal tract in medicine?
Prokinetic drugs that stimulate upper gastrointestinal motility are helpful for gastroparesis and for postsurgical gastric emptying delay. Their ability to increase lower esophageal sphincter pressures also makes them useful for some patients with GERD.
What are proton pump inhibitors used for in the digestive system?
What kind of medications are used to cleanse the stomach?

What is the most effective treatment for gastroesophageal reflux disease?
1. Gastroesophageal reflux disease — PPI s are the most effective agents for the treatment of nonerosive and erosive reflux disease, esophageal complications of reflux disease (peptic stricture or Barrett’s esophagus), and extraesophageal manifestations of reflux disease. Once-daily dosing provides effective symptom relief and tissue healing in 85–90% of patients; up to 15% of patients require twice-daily dosing.
How does the gastroduodenal mucosa protect itself from acid and pepsin?
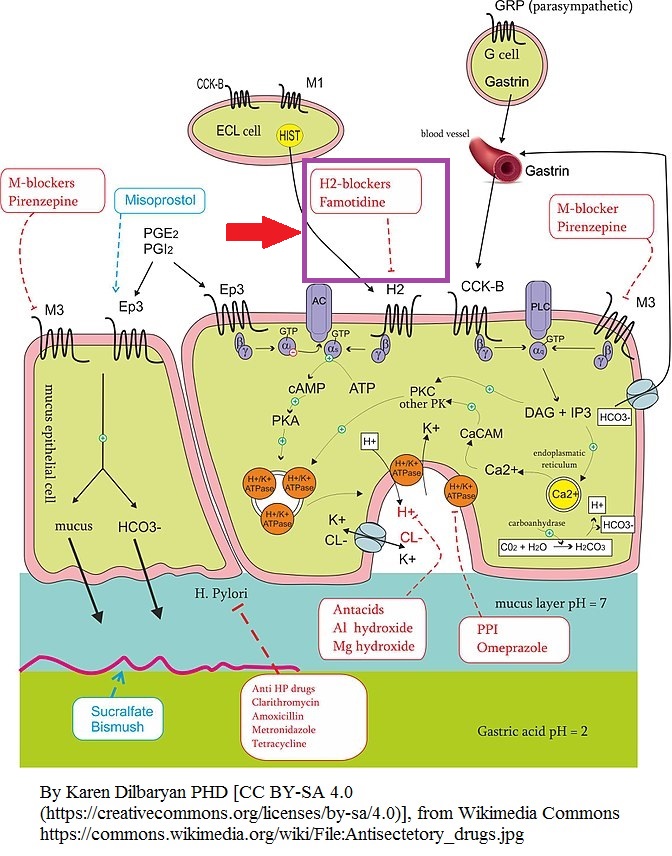
Both mucus and epithelial cell-cell tight junctions restrict back diffusion of acid and pepsin. Epithelial bicarbonate secretion establishes a pH gradient within the mucous layer in which the pH ranges from 7 at the mucosal surface to 1–2 in the gastric lumen. Blood flow carries bicarbonate and vital nutrients to surface cells. Areas of injured epithelium are quickly repaired by restitution, a process in which migration of cells from gland neck cells seals small erosions to reestablish intact epithelium. Mucosal prostaglandins appear to be important in stimulating mucus and bicarbonate secretion and mucosal blood flow. A number of agents that potentiate these mucosal defense mechanisms are available for the prevention and treatment of acid-peptic disorders.
How old is a woman with Crohn's disease?
A 21-year-old woman comes with her parents to discuss therapeutic options for her Crohn’s disease. She was diagnosed with Crohn’s disease 2 years ago, and it involves her terminal ileum and proximal colon, as confirmed by colonoscopy and small bowel radiography. She was initially treated with mesalamine and budesonide with good response, but over the last 2 months, she has had a relapse of her symptoms. She is experiencing fatigue, cramping, abdominal pains, and nonbloody diarrhea up to 10 times daily, and she has had a 15-lb weight loss.
What causes peptic ulcers?
Over 90% of peptic ulcers are caused by infection with the bacterium Helicobacter pylori or by use of nonsteroidal anti-inflammatory drugs (NSAIDs). Drugs used in the treatment of acid-peptic disorders may be divided into two classes: agents that reduce intragastric acidity and agents that promote mucosal defense.
When were PPIs first used?
Since their introduction in the late 1980s, these efficacious acid inhibitory agents have assumed the major role for the treatment of acid-peptic disorders. PPIs are now among the most widely prescribed drugs worldwide due to their outstanding efficacy and safety.
What receptors are in the parietal cell?
The parietal cell contains receptors for gastrin (CCK-B), histamine (H 2 ), and acetylcholine (muscarinic, M 3) ( Figure 62–1 ). When acetylcholine (from vagal postganglionic nerves) or gastrin (released from antral G cells into the blood) bind to the parietal cell receptors, they cause an increase in cytosolic calcium, which in turn stimulates protein kinases that stimulate acid secretion from a H + /K + -ATPase (the proton pump) on the canalicular surface.
How often is sucralfate given?
Sucralfate is administered in a dosage of 1 g four times daily on an empty stomach (at least 1 hour before meals). At present, its clinical uses are limited. Sucralfate (administered as a slurry through a nasogastric tube) reduces the incidence of clinically significant upper gastrointestinal bleeding in critically ill patients hospitalized in the intensive care unit, although it is slightly less effective than intravenous H 2 antagonists. Sucralfate is still used by many clinicians for prevention of stress-related bleeding because of concerns that acid inhibitory therapies (antacids, H 2 antagonists, and PPIs) may increase the risk of nosocomial pneumonia.
What is the best medicine for gastrointestinal problems?
For example, indigestion and acid reflux can be treated with antacids or medicines such as omeprazole and ranitidine. Symptoms of irritable bowel syndrome (IBS) can be relieved with mebeverine or hyoscine.
How long does irritable bowel syndrome last?
Ask a pharmacist for advice on which medicines are most suitable for you. If any gastrointestinal symptoms are worrying or last longer than about two weeks, make an appointment to see your doctor.
What are the functions of the gastrointestinal tract?
The gastrointestinal tract serves many important functions: digestive, excretory, endocrine, exocrine, and so on. These functions are the targets of several important classes of drugs. Some of these drugs have been discussed previously.
What is the medical term for inflammation of the colon?
Inflammatory bowel disease (IBD) Inflammatory disorder involving irritation and ulceration of the colon and rectum (ulcerative colitis) or the colon plus more proximal parts of the gastrointestinal tract (Crohn’s disease) Irritable bowel syndrome (IBS)
What is acid peptic disease?
Acid-peptic disease. A group of disorders involving erosion or ulceration of the mucosal lining of the gastrointestinal tract; includes GERD, gastric and duodenal ulcers, nonulcer dyspepsia, and stress-related gastritis. Antiemetic. A drug that reduces nausea and vomiting. Gastroesophageal reflux disease (GERD)

Introduction
Drugs Used in Acid-Peptic Diseases
- Acid-peptic diseases include gastroesophageal reflux, peptic ulcer (gastric and duodenal), and stress-related mucosal injury. In all these conditions, mucosal erosions or ulceration arise when the caustic effects of aggressive factors (acid, pepsin, bile) overwhelm the defensive factors of the gastrointestinal mucosa (mucus and bicarbonate secretio...
Physiology of Acid Secretion
- The parietal cell contains receptors for gastrin (CCK-B), histamine (H2), and acetylcholine (muscarinic, M3) (Figure 62–1). When acetylcholine (from vagal postganglionic nerves) or gastrin (released from antral G cells into the blood) bind to the parietal cell receptors, they cause an increase in cytosolic calcium, which in turn stimulates protein kinases that stimulate acid secreti…
Antacids
- Antacids have been used for centuries in the treatment of patients with dyspepsia and acid-peptic disorders. They were the mainstay of treatment for acid-peptic disorders until the advent of H2−receptor antagonists and proton-pump inhibitors (PPIs). They continue to be used commonly by patients as nonprescription remedies for the treatment of intermittent heartburn and dyspeps…
H2-receptor Antagonists
- From their introduction in the 1970s until the early 1990s, H2-receptor antagonists (commonly referred to as H2 blockers) were the most commonly prescribed drugs in the world (see Clinical Uses). With the recognition of the role of H pylori in ulcer disease (which may be treated with appropriate antibacterial therapy) and the advent of PPIs, the use of prescription H2blockers ha…
Chemistry & Pharmacokinetics
- Four H2 antagonists are in clinical use: cimetidine, ranitidine, famotidine, and nizatidine. All four agents are rapidly absorbed from the intestine. Cimetidine, ranitidine, and famotidine undergo first-pass hepatic metabolism resulting in a bioavailability of approximately 50%. Nizatidine has little first-pass metabolism. The serum half-lives of the four agents range from 1.1 to 4 hours; ho…
Pharmacodynamics
- The H2 antagonists exhibit competitive inhibition at the parietal cell H2 receptor and suppress basal and meal-stimulated acid secretion (Figure 62–2) in a linear, dose-dependent manner. They are highly selective and do not affect H1 or H3 receptors (see Chapter 16). The volume of gastric secretion and the concentration of pepsin are also reduced. FIGURE 62–2 Twenty-four-hour med…
Clinical Uses
- H2-receptor antagonists continue to be prescribed but PPIs (see below) are steadily replacing H2 antagonists for most clinical indications. However, the over-the-counter preparations of the H2antagonists are heavily used by the public. 1. Gastroesophageal reflux disease (GERD)—Patients with infrequent heartburn or dyspepsia (fewer than 3 times per week) may tak…
Adverse Effects
- H2 antagonists are extremely safe drugs. Adverse effects occur in less than 3% of patients and include diarrhea, headache, fatigue, myalgias, and constipation. Some studies suggest that intravenous H2antagonists (or PPIs) may increase the risk of nosocomial pneumonia in critically ill patients. Mental status changes (confusion, hallucinations, agitation) may occur with adminis…
Drug Interactions
- Cimetidine interferes with several important hepatic cytochrome P450 drug metabolism pathways, including those catalyzed by CYP1A2, CYP2C9, CYP2D6, and CYP3A4 (see Chapter 4). Hence, the half-lives of drugs metabolized by these pathways may be prolonged. Ranitidine binds 4–10 times less avidly than cimetidine to cytochrome P450. Negligible interaction occurs with ni…