Are inhaled corticosteroids effective in the treatment of asthma?
Sep 27, 2019 · In short, corticosteroids lower the inflammation in the body and, specifically for asthmatics, in the lungs. Corticosteroids mimic the hormones that are produced naturally in the body (more specifically the adrenal glands). When the dose is more than what the body naturally makes, it suppresses inflammation. The SET mnemonic for asthma
When should inhaled corticosteroids be added to bronchodilators?
It is beyond any doubt that CS act on many sites to help reverse the pathologic process of bronchial asthma. Corticosteroids enhance the beta-adrenergic response to relieve the muscle spasm. They also act by reversing the mucosal edema, decreasing vascular permeability by vasoconstriction, and inhibiting the release of LTC4 and LTD4.
What are inhaled corticosteroids (ICS)?
Inhaled corticosteroids are extremely useful in management of asthma poorly controlled with bronchodilators, and physicians may consider adding them to bronchodilators from the earliest phases of therapeutic intervention for adult asthma. A practical guide to the use of inhaled corticosteroids in asthma is presented. Publication types Review
Which medications are used in the treatment of asthma exacerbations?
Inhaled corticosteroids have a proven benefit in the management of asthma, but until recently, their efficacy in non-asthmatic, smoking-related chronic obstructive pulmonary disease (COPD) was not evidence-based. Airway inflammation in COPD differs from inflammation in asthma. Some studies have shown an effect of inhaled corticosteroids on airway inflammation in COPD …

Why do you need an oral corticosteroid for asthma?
Oral corticosteroids (OCS) When our asthma is flaring up and our daily maintenance ICS aren’t enough to keep asthma symptoms at bay, your doctor may put you on an oral corticosteroid for a short period of time to decrease the amount of inflammation in the lungs.
What are the three forms of corticosteroids?
Corticosteroids have become center stage in the treatment and prevention of asthma exacerbations. They come in three forms: oral, inhaled, and intravenous (IV).
What does "set" mean in asthma?
When providing education for asthmatics, in the respiratory field we use the SET mnemonic. SET stands for S welling, E xcess mucus, and T ightness. These are the three main things that happen during an asthma flare-up or asthma attack. Inflammation in the lungs is what causes the swelling which makes it difficult to breathe. Mucus production is increased and when combined with the swelling and tightness, causes wheezing. Tightness happens from both the swelling and bronchospasm. These three things create a perfect storm when you are exposed to a trigger.
Can asthma be controlled without breathing?
Not everyone will experience the same side effects and some might not experience any at all. You will have to weigh the options with your doctor and decide what is the best course of action for your specific asthma. While the side effects may be unpleasant, not being able to breathe is far worse. Being able to keep your asthma controlled without ...
Do corticosteroids cause inflammation?
Corticosteroids mimic the hormones that are produced naturally in the body (more specifically the adrenal glands). When the dose is more than what the body naturally makes, it suppresses inflammation.
Can you use OCS for asthma?
Being able to keep your asthma controlled without excessive use of OCS is ideal. However in rare cases, there is a need for long term daily OCS due to asthma severity. Long term use of OCS can lead to some serious problems including decreased bone density, diabetes, and adrenal fatigue.
What are the limitations of corticosteroids?
The limitation of using corticosteroids are their side effects. They vary from tolerable to life threatening side effects. Each tissue in the body is a target for corticosteroids. The mechanism of adverse effects have been studied in extensive detail but many questions are yet to be answered.
How do corticosteroids help with muscle spasms?
Corticosteroids enhance the beta-adrenergic response to relieve the muscle spasm. They also act by reversing the mucosal edema, decreasing vascular permeability by vasoconstriction, and inhibiting the release of LTC4 and LTD4. Corticosteroids reduce the mucus secretion by inhibiting the release of secretagogue from macrophages.
How do corticosteroids affect mucus secretion?
Corticosteroids reduce the mucus secretion by inhibiting the release of secretagogue from macrophages. Corticosteroids inhibit the late phase reaction by inhibiting the inflammatory response and interfering with chemotaxis. This action may be due to the inhibition of LTB4 release.
Do corticosteroids cause bronchial reactivity?
Corticosteroids have no effect on the immediate hypersensitivity reaction and have no direct role in bronchial reactivity. By blocking the late reaction, they prevent the increased airway reactivity observed with late bronchial reactions. The limitation of using corticosteroids are their side effects.
Do corticosteroids help with asthma?
It is beyond any doubt that CS act on many sites to help reverse the pathologic process of bronchial asthma. Corticosteroids enhance the beta-adrenergic response to relieve the muscle spasm. They also act by reversing the mucosal edema, decreasing vascular permeability by vasoconstriction, and inhibiting the release of LTC4 and LTD4. Corticosteroids reduce the mucus secretion by inhibiting the release of secretagogue from macrophages. Corticosteroids inhibit the late phase reaction by inhibiting the inflammatory response and interfering with chemotaxis. This action may be due to the inhibition of LTB4 release. The eosinopenic effect of corticosteroids may help to prevent the cytotoxic effect of the major basic protein and other inflammatory mediators released from eosinophils. Corticosteroids have no effect on the immediate hypersensitivity reaction and have no direct role in bronchial reactivity. By blocking the late reaction, they prevent the increased airway reactivity observed with late bronchial reactions. The limitation of using corticosteroids are their side effects. They vary from tolerable to life threatening side effects. Each tissue in the body is a target for corticosteroids. The mechanism of adverse effects have been studied in extensive detail but many questions are yet to be answered. Alternate-day therapy and inhalation therapy are meant to minimize these side effects. The expansion of using inhaled steroid therapy and finding some inhaled preparations that have even less systemic side effects seems a reasonable approach to deal with severe asthma.
How often should I take hydrocortisone?
Analysis of these studies suggests that hydrocortisone (4 mg/kg) or methylprednisolone (125 mg) as the initial dose, followed by a continuous infusion of hydrocortisone (12 mg/kg over 24 hours), or bolus injections of methylprednisolone (125 mg every 6 hours) may be the most appropriate corticosteroid therapy in acute asthma.
Is methylprednisolone better than hydrocortisone?
Methylprednisolone may have some pharmacologic advantages over hydrocortisone. A clinical approach to tapering of corticosteroids after treatment of an acute exacerbation is outlined. Hypothalamic-pituitary-adrenal-axis suppression with chronic oral and inhaled corticosteroid use and the management of corticosteroid therapy in such patients are ...
Can corticosteroids be used for asthma?
Inhaled corticosteroids are extremely useful in management of asthma poorly controlled with bronchodilators, and physicians may consider adding them to bronchodilators from the earliest phases of therapeutic intervention for adult asthma.
How do corticosteroids affect the airway?
These effects of corticosteroids are produced through inhibiting the recruitment of inflammatory cells into the airway by suppressing the production of chemotactic mediators and adhesion molecules and by inhibiting the survival in the airways of inflammatory cells , such as eosinophils, T-lymphocytes and mast cells.
What is the main action of corticosteroids?
The major action of corticosteroids is to switch off multiple activated inflammatory genes that encode for cytokines, chemokines, adhesion molecules inflammatory enzymes and receptors [1].
What is the most effective control for asthma?
Introduction. Inhaled corticosteroids (ICS, also known as glucocorticosteroids, glucocorticoids, steroids) are by far the most effective controllers used in the treatment of asthma and the only drugs that can effectively suppress the characteristic inflammation in asthmatic airways, even in very low doses.
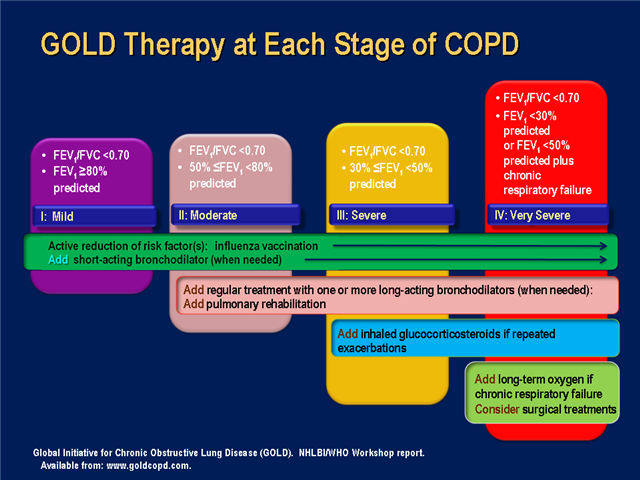
Why are ICS added to bronchodilators?
ICS are added to bronchodilators in patients with severe COPD to reduce exacerbations.
How effective is ICS?
ICS are very effective in controlling asthma symptoms in asthmatic patients of all ages and severity. ICS improve the quality of life of patients with asthma and allow many patients to lead normal lives, improve lung function, reduce the frequency of exacerbations and may prevent irreversible airway changes.
What are some examples of genes that are activated by corticosteroids?
Examples of genes that are activated by corticosteroids include genes encoding β2-adrenergic receptors and the anti-inflammatory proteins secretory leukoprotease inhibitor and mitogen-activated protein kinase phosphatase-1 (MKP-1) which inhibits MAP kinase pathways.
What is the target of ICS?
Epithelial cells may be a major cellular target for ICS, which are the mainstay of modern asthma management. ICS suppress many activated inflammatory genes in airway epithelial cells (Figure 2). Epithelial integrity is restored by regular ICS.
What is corticosteroids used for?
Both can be used medicinally to treat a variety of health conditions, including orthopedic conditions like arthritis and inflammation from soft tissue injuries.
How do corticosteroids affect the body?
Glucocorticoids can help to fight inflammation and suppress hypersensitive white blood cell responses to infection and other threats. These corticosteroids also affect blood pressure and skin cell production .
Why are corticosteroids dangerous?
The very reasons they work so well at reducing pain and inflammation are the same reasons they’re dangerous if taken too frequently or in large quantities. Corticosteroids suppress the immune system and the creation of white blood cells, halting immune system “overreactions” that create pain and swelling .
Why do orthopedists inject corticosteroids?
In orthopedics, injectable corticosteroids are often used for their anti-inflammatory properties. For some painful conditions, for example arthritis or a bulging disc, an orthopedist may suggest one or more injections to the joint or the site of injury in order to bring down swelling, inflammation, or pain.
Why does my neck hurt?
Neck pain (cervical radiculopathy). A pinched nerve in the neck vertebrae can lead to a radiating pain felt in the neck, shoulder, arm, or even the hands. This pinching can be caused by a compression of the vertebrae, a bulging disc, or a ruptured disc. A corticosteroid injection can bring down the swelling while the injury heals.
What is the treatment for osteoarthritis?
Aspiration of collected fluid, followed by corticosteroid injection is an option for treatment. Osteoarthritis (OA). Treatment of OA is probably one of the most common uses of corticosteroids in orthopedics. When cartilage wears away, pain and inflammation in the joints is common.
What causes pain in the tendons and soft tissues?
Tendonitis. This inflammatory condition — often the result of overuse or repetitive strain — can lead to pain and swelling in the tendons and soft tissues. Tendonitis is especially common in the elbow (tennis elbow), the shoulders, the knees, and the wrists. Injections may bring some relief from severe or disabling pain.
What is the best treatment for asthma?
For individuals with mild persistent asthma, either of the following two treatments are recommended as part of Step 2 therapy: 1) a daily low-dose ICS and as-needed SABA for quick-relief therapy, or 2) intermittent as-needed SABA and ICS used one after the other for worsening asthma.
What is the focus of the 2020 Asthma Management Guidelines?
This Clinician’s Guide summarizes the 2020 Focused Updates to the Asthma Management Guidelines: A Report from the National Asthma Education and Prevention Program Coordinating Committee Expert Panel Working Group to help clinicians integrate the new recommendations into clinical care. The full 2020 Report, which is focused on selected topics rather than a complete revision of the 2007 Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma (EPR-3), can be found at nhlbi.nih.gov/asthmaguidelines. This summary guide should be used in conjunction with the full report. The Guide is organized by the following topics:
What is SCIT used for?
SCIT is recommended as an adjunct treatment for individuals who have demonstrated allergic sensitization and evidence of worsening asthma symptoms after exposure to the relevant antigen or antigens.
What is ICS therapy?
Scheduled, daily inhaled corticosteroid (ICS) treatment is the currently preferred pharmacologic controller therapy for persistent asthma in individuals of all ages. Intermittent ICS dosing includes courses of ICS treatment used for brief periods, usually in response to symptoms or as an add-on with or without a long-acting beta2-agonist (LABA). Recommendations for ICS treatment are organized by age.
How old do you have to be to take ICS?
In individuals ages 12 years and older with mild persistent asthma, the Expert Panel conditionally recommends either daily low-dose ICS and as-needed SABA for quick-relief therapy or as-needed ICS and SABA used concomitantly.
When should I use FeNO?
In individuals ages 5 years and older with persistent allergic asthma, for whom there is uncertainty in choosing, monitoring, or adjusting anti-inflammatory therapies based on history, clinical findings, and spirometry, the Expert Panel conditionally recommends the addition of FeNO measurement as part of an ongoing asthma monitoring and management strategy that includes frequent assessments.
When to use subcutaneous immunotherapy?
In individuals ages 5 years and older with mild to moderate allergic asthma , the Expert Panel conditionally recommends the use of subcutaneous immunotherapy as an adjunct treatment to standard pharmacotherapy in those individuals whoseasthma is controlled at the initiation, build up, and maintenance phases of immunotherapy.
What is the best treatment for asthma?
If you have serious worsening of asthma symptoms (an asthma attack), your doctor may prescribe a brief course of oral steroids such as prednisone. Oral steroids may also be prescribed when your asthma symptoms worsen but you do not require hospitalization.
What are the side effects of asthma inhalers?
Unlike the serious side effects of oral steroids, the most common side effects of anti-inflammatory asthma inhalers are hoarseness and thrush, ...
Does prednisone go through the body?
That means that after taking prednisone by mouth (orally), it is absorbed in the body, unlike inhaled steroids (anti-inflammatory asthma inhalers) that go straight to the lungs. Prednisone decreases your immune system's response to reduce symptoms such as swelling and allergic-type reactions. Prednisone and other systemic steroids may be used ...
Can you take steroids for asthma?
Steroids, anti-inflammatory drugs such as prednisone, can be used for asthma as well as other lung diseases. Prednisone and other steroids (inhaled, oral, or by injection) help calm airway inflammation in asthma. If you've ever had a serious asthma attack, you may have had high doses of steroids administered intravenously in the hospital.
Should I rinse my mouth after using an asthma inhaler?
As with all asthma inhalers, you should rinse the mouth carefully after using your inhaler. Gargle with water after inhalation to help reduce the risk of oral thrush. For more detail, see WebMD’s Asthma, Steroids & Other Anti-Inflammatory Drugs. Share on Facebook Share on Twitter Share on Pinterest Email Print.
Can you take prednisone every day?
This is called a steroid burst. They may also be given in a low dose daily or every other day for long-term asthma control .