- Intravenous fluids. Your doctor may recommend IV sodium solution to slowly raise the sodium levels in your blood. ...
- Medications. You may take medications to manage the signs and symptoms of hyponatremia, such as headaches, nausea and seizures.
What is the mainstay of treatment for SIADH?
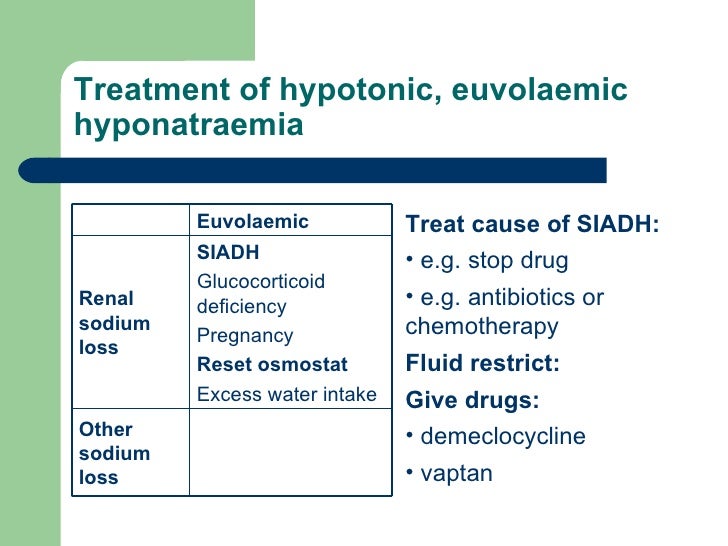
Fluid restriction is the mainstay of treatment for SIADH; however, the degree of restriction necessary will vary, depending on the patient's ability to excrete electrolyte‐free water.
What happens if sodium is low in SIADH?
A low sodium level or hyponatremia is a major complication of SIADH and is responsible for many of the symptoms of SIADH. Early symptoms may be mild and include cramping, nausea, and vomiting. In severe cases, SIADH can cause confusion, seizures, and coma.
When should hypertonic saline be used in the treatment of SIADH?
This is most likely to occur if urinary osmolality is above 530 mOsm/kg, as some patients with SIADH and lower urinary osmolalities have been successfully treated with isotonic saline [ 15 ]. If a patient is symptomatic due to a rapid decrease in serum sodium concentration, treatment with hypertonic saline should be considered [ 16 ].
Is fluid restriction effective in the treatment of SIADH?
Although fluid restriction was helpful in the first patients described with SIADH [Schwartz et al. 1957] and is generally recommended [Berl and Robertson, 2000] in everyday practice it may be difficult to impose and frustrating to control. Whenever possible, treatment of an underlying pathology of SIADH can be expected to correct hyponatremia.
How do you fix sodium in SIADH?
In patients with severe symptomatic hyponatremia, the rate of sodium correction should be 6 to 12 mEq per L in the first 24 hours and 18 mEq per L or less in 48 hours. A bolus of 100 to 150 mL of hypertonic 3% saline can be given to correct severe hyponatremia.
What is the best treatment for SIADH?
The most commonly prescribed treatment for SIADH is fluid and water restriction. If the condition is chronic, fluid restriction may need to be permanent. Treatment may also include: Certain medications that inhibit the action of ADH (also called vasopressin)
What IV fluids are used to treat hyponatremia?
The most common treatment option proposed for patients with hypovolemic hyponatremia is replacement of both salt and water through the intravenous infusion of sodium chloride solutions.
What is the initial treatment for hyponatremia?
For serious symptomatic hyponatremia, the first line of treatment is prompt intravenous infusion of hypertonic saline, with a target increase of 6 mmol/L over 24 hours (not exceeding 12 mmol/L) and an additional 8 mmol/L during every 24 hours thereafter until the patient's serum sodium concentration reaches 130 mmol/L.
How do you raise the sodium level in your blood?
TreatmentIntravenous fluids. Your doctor may recommend IV sodium solution to slowly raise the sodium levels in your blood. ... Medications. You may take medications to manage the signs and symptoms of hyponatremia, such as headaches, nausea and seizures.
Do you restrict fluids with SIADH?
Fluid restriction is first-line therapy in all cases of SIADH. Where hyponatraemia has persisted for longer than 48 hours and is asymptomatic, initial fluid restriction could start at 800–1200 mL per 24 hours, and be subsequently titrated to 500 mL below the daily urine output volume.
What medications increase sodium levels?
Drug Induced HypernatraemiaDiuretics.Sodium bicarbonate.Sodium chloride.Corticosteroids.Anabolic steroids.Adrenocorticotrophic steroids.Androgens.Oestrogens.
Why do you give hypertonic saline for Siadh?
Oral salt tablets can be used in patients with mild-moderate hyponatremia. When using intravenous saline, the electrolyte concentration of the administered fluid must be greater than the electrolyte concentration of the urine. This usually requires the use of hypertonic saline.
Is LR or NS better for hyponatremia?
In both studies, there was significantly more hyponatremia associated with balanced solutions in comparison to normal saline, which is likely due to the use of lactated Ringer's. In the SALT-ED, 95 percent of patients received lactated Ringer's, and the serum sodium fell (p <0.001).
What happens if you correct low sodium too quickly?
But new evidence shows that when patients with hyponatremia get admitted to the hospital, their impatient treatment teams often correct sodium levels too quickly, increasing the risk for dangerous complications. Too-rapid correction of sodium can cause osmotic demyelination syndrome (ODS), a form of brain damage.
What fluid order do you expect for the treatment of hyponatremia in a patient who is Normovolemic?
Acute normovolemic hyponatremia is treated by the intravenous administration of 3% NaCl and with the simultaneous use of loop diuretics (20- 40 mg Furosemide/ 24 hrs) and restriction of fluid intake.
What IV fluid is best for Hypernatremia?
Patients should be given intravenous 5% dextrose for acute hypernatremia or half-normal saline (0.45% sodium chloride) for chronic hypernatremia if unable to tolerate oral water.
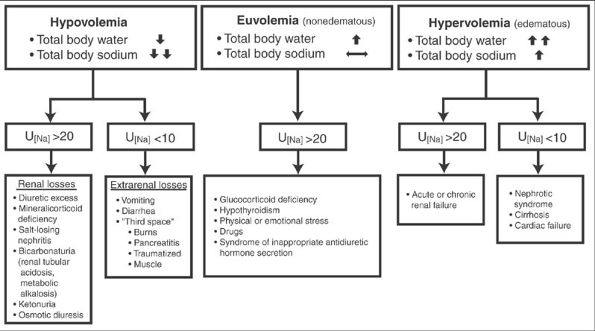
What is the syndrome of inappropriate antidiuretic hormone secretion?
The syndrome of inappropriate antidiuretic hormone secretion (SIADH), the oft‐quoted cause of hyponatraemia by medical students, is a diagnosis of exclusion that , by definition, is associated with a normal volume status.
Is hyponatraemia asymptomatic or asymptomatic?
The majority of cases of hyponatraemia are mild, and it is generally thought of as an asymptomatic condition, although even mild hyponatraemia may have detrimental effects on patients 2, 3. The symptoms of hyponatraemia are nonspecific in the majority, and hyponatraemia is often discovered coincidentally.
What is the best treatment for SIADH?
Treatment and prognosis for SIADH. The first line of treatment is to limit fluid intake to avoid further buildup. Medications may include those that can reduce fluid retention, such as furosemide (Lasix), and those that can inhibit ADH, like demeclocycline. Your prognosis will depend on the cause of SIADH.
How to know if you have SIADH?
Early symptoms may be mild and include cramping, nausea, and vomiting. In severe cases, SIADH can cause confusion, seizures, and coma. Treatment usually begins with limiting fluid intake to prevent further buildup. Additional treatment will depend on the cause.
What is the normal ADH level?
According to the University of Rochester Medical Center, normal values for ADH range from 0-5 picograms per milliliter. Higher levels could be the result of SIADH.
What are the criteria for SIADH?
A set of criteria was created in 1967 by William Schwartz and Frederic Bartter for the diagnosis of SIADH that are still in use today. These criteria are: 1 Serum sodium less than 135mEq/L 2 Serum osmolality less than 275 mOsm/kg 3 Urine sodium over 40 mEq/L 4 Urine osmolality over 100 mOsm/kg 5 No evidence of volume depletion 6 No evidence of other causes of low sodium levels, such as hyperthyroidism, cardiac failure, kidney disease, or pituitary gland problems 7 Sodium levels improve with fluid restriction.
Why does dilute blood cause SIADH?
This leads to symptoms of SIADH, which occur because of the low levels of sodium in the blood.
What is the mechanism of siadh?
Mechanism of SIADH. The mechanism by which SIADH develops primarily involves the kidneys. Inside the kidneys are tubes called nephrons that move fluid and waste along to the bladder and control how much water leaves the body.
What is the syndrome of inappropriate antidiuretic hormone secretion?
Syndrome of inappropriate antidiuretic hormone secretion (SIADH) is a condition in which there are high amounts of antidiuretic hormone (ADH) released from the pituitary gland or other sources. Image Credit: Yeexin Richelle/Shutterstock.com.
What causes low sodium levels in the blood?
Syndrome of inappropriate antidiuretic hormone secretion causes low sodium levels in the blood through excessive water retention. The extra water diluting the blood lowers the amounts of certain electrolytes in the blood and can cause serious symptoms such as seizures, coma, and psychological symptoms such as mood changes and hallucinations.
What are the different types of SIADH?
There are four types of SIADH: type A, B, C, and D . Type A occurs independently of plasma osmolality. There are high levels of ADH and urine osmolality. Type B is characterized by a constant release of ADH. Type C is characterized by a baseline plasma sodium concentration that is stable, but lower than normal. ...
Where is antidiuretic hormone produced?
Antidiuretic hormone is also called arginine vasopressin (AVP). It is produced in the hypothalamus in the brain. ADH has been found to help to regulate the osmotic balance in the body, which refers to the amounts of electrolytes and non-electrolytes in the cells, tissues, and interstitial fluid. It also regulates sodium levels, blood pressure, ...
How to treat hyponatremia?
If you have severe, acute hyponatremia, you'll need more-aggressive treatment. Options include: 1 Intravenous fluids. Your doctor may recommend IV sodium solution to slowly raise the sodium levels in your blood. This requires a stay in the hospital for frequent monitoring of sodium levels as too rapid of a correction is dangerous. 2 Medications. You may take medications to manage the signs and symptoms of hyponatremia, such as headaches, nausea and seizures.
What to do if you have a headache and nausea?
Preparing for your appointment. Seek emergency care for anyone who develops severe signs and symptoms of hyponatremia, such as nausea and vomiting, confusion, seizures, or lost consciousness. Call your doctor if you know you are at risk of hyponatremia and are experiencing nausea, headaches, cramping or weakness.
Can you take medication for hyponatremia?
Medications. You may take medications to manage the signs and symptoms of hyponatremia, such as headaches, nausea and seizures.
Can you cut back on fluids with hyponatremia?
Hyponatremia treatment is aimed at addressing the underlying cause, if possible. If you have moderate, chronic hyponatremia due to your diet, diuretics or drinking too much water, your doctor may recommend temporarily cutting back on fluids.
Can a doctor diagnose hyponatremia?
However, because the signs and symptoms of hyponatremia occur in many conditions, it's impossible to diagnose the condition based on a physical exam alone.
What are the symptoms of SIADH?
Symptoms. Symptoms of SIADH vary depending upon both the severity of the hyponatraemia and the rate at which it develops: Mild hyponatraemia: nausea, vomiting, headache, anorexia and lethargy. Moderate hyponatraemia: muscle cramps, weakness, confusion and ataxia. Severe hyponatraemia: drowsiness, seizures and coma.
What is SIADH in medical terms?
What is SIADH? The syndrome of inappropriate antidiuretic hormone secretion (SIADH) is characterised by excessive secretion of antidiuretic hormone (ADH) from the posterior pituitary gland or another source.
How does ADH affect water retention?
ADH controls water reabsorption via its effect on kidney nephrons, causing the retention of water (but not the retention of solutes). By increasing water retention, ADH assists in the dilution of the blood, decreasing the concentration of solutes such as sodium.
What is the difference between normal physiology and what occurs in SIADH?
Deranged physiology in SIADH. The important difference between normal physiology and what occurs in SIADH is the lack of an effective negative feedback mechanism. This results in continual ADH production, independent of serum osmolality.
Where is ADH released?
2. ADH is transported from the hypothalamus to the posterior pituitary gland. 3. ADH is released into the circulatory system via the posterior pituitary gland. 4.
Can TFTs cause SIADH?
TFTs: Hypothyroidism is a potential cause of SIADH. Reduced T3 and raised TSH would suggest this diagnosis. Serum cortisol: should be checked to rule out Addison’s disease as a cause of hyponatraemia (cortisol is reduced in Addison’s disease).
Can SIADH cause low sodium levels?
Mild hyponatraemia may cause significant symptoms if the drop in sodium is acute, whereas chronically hyponatraemic patients may have very low serum sodium concentrations and yet be completely asymptomatic.
What is the osmolality of saline in SIADH?
As urine osmolality in SIADH frequently ranges from 400–600 mOsmol/kg, infusion with isotonic saline may lead to a further decrease in serum osmolality. A frequent misconception is that isotonic saline (300 mOsmol/kg) is hypertonic to the patient and should therefore lead to correction of hyponatraemia. However, when the infusate (Na) is lower than the patient's urinary (Na + K), the use of isotonic saline represents a source of free water. This process is referred to as desalination [ 14 ]. This is most likely to occur if urinary osmolality is above 530 mOsm/kg, as some patients with SIADH and lower urinary osmolalities have been successfully treated with isotonic saline [ 15 ].
Does lithium cause NDI?
Like demeclocycline, lithium carbonate causes NDI in some 65% of patients. Patients with bipolar disorder generally respond well to lithium treatment, but the side effects on urinary concentrating ability often cause polyuria and polydipsia. Lithium appears to enter the principal cells of the collecting duct through the epithelial sodium channel ENaC and reduces aquaporin-2 expression [ 29 ]. Long-term treatment with lithium may induce tubulo-interstitial nephritis that can lead to irreversible NDI and end-stage renal failure [ 30 ]. The effect of lithium takes approximately 4 days to set in. The serum lithium concentration must be followed closely in order to prevent renal toxicity. For these reasons, the use of lithium to treat SIADH has been mostly abandoned. In animal models, however, lithium has been shown to augment the effects of aquaretic agents [ 31 ].
Can vaptans increase sodium?
If vaptans were to be proven to lead to a more predictable rise in serum sodium concentrations, either as initial treatment or as sequential treatment following hypertonic saline, with greater effectiveness compared to fluid restriction, this could potentially reduce the length of hospitalization and thereby cost.
Is vasopressin low in SIADH?
In these patients plasma vasopressin levels are low or even undetectable at all levels of serum osmolality. Not all patients with drug-induced SIADH have measurable plasma levels of vasopressin, suggesting that modulation of the vasopressin-receptor aquaporin-2 signalling pathway may also occur [ 5 ].
Is SIADH a treatment for hyponatraemia?
The treatment of hyponatraemia due to SIADH is not always as straightforward as it seems. Although acute treatment with hypertonic saline and chronic treatment with fluid restriction are well established, both approaches have severe limitations.
Can vaptans be used for hyponatraemia?
Many more questions need to be answered before one can make well-founded recommendations for the use of vaptans in treating patients with hypo natraemia due to SIADH. Future trials should address the possible superiority of vaptans to hypertonic saline in treating acute hyponatraemia. In chronic treatment, the advantages in terms of effectiveness and quality of life, as compared to water restriction, certainly require further study. However, as some of these agents are now registered for the treatment of euvolaemic hyponatraemia, one can only hope treating physicians will apply these drugs with the same amount of care as exhibited in patients that were included in the recent trials.