What is the continuation phase of treatment for tuberculosis (TB)?
The continuation phase of treatment is given for either 4- or 7- months. Daily or three times weekly therapy is the recommended therapy. The 4-month continuation phase should be used in Patients with uncomplicated, non-cavitary, drug-susceptible TB, if there is documented sputum culture conversion within the first 2 months.
How long does it take to cure TB?
This means that the person is then cured of TB. But TB bacteria die very slowly, and so the drugs have to be taken for several months. Even when a patient starts to feel better they can still have bacteria alive in their body. So the person needs to keep taking the drugs until all the bacteria are dead.
What is the initial initial anti-TB regimen for Class 3 tuberculosis (TB)?
The standard initial anti-TB regimen for class 3 or class 5 patients consists of a four-drug regimen of INH, RIF, PZA, and ethambutol (EMB), unless otherwise contraindicated. Streptomycin (SM) may be substituted for EMB, but because of greater toxicity and intramuscular administration, it should be used only when EMB is contraindicated.
What is the first line treatment for tuberculosis (TB) infection?
If the bacteria that they are infected with are not resistant to any of the first line drugs then the standard first line treatment of 2HRZE/4HR can be repeated. If there is resistance then an MDR-TB regimen should be prescribed according to WHO's guidance for the treatment of drug resistant TB.
Why are TB drugs given for several months?
After taking antibiotics for 2 weeks, most people are no longer infectious and feel better. However, it's important to continue taking your medicine exactly as prescribed and to complete the whole course of antibiotics. Taking medication for 6 months is the best way to ensure the TB bacteria are killed.
How long is the initial phase of TB treatment?
Individuals with central nervous system tuberculosis should be offered standard treatment with initial phase drugs for 2 months (see Initial phase for specific drugs).
Can TB be cured in 2 months?
TB treatment takes at least six months, patients need to take many tablets each day and side effects are common.
Why antibiotic treatment for TB takes a long time?
Latent TB Infection The goal of this treatment is to eliminate the bacteria from your body. A long treatment is required because antibiotics work only when the bacteria are actively dividing, and the bacteria that cause TB can rest without growing for long periods.
What are the phases of TB treatment?
Treatment for TB DiseaseIntensive PhaseContinuation PhaseDrugsaDurationDurationINH RIF PZA EMB8 weeks18 weeksINH RIF PZA EMB8 weeks18 weeksINH RIF PZA EMB8 weeks18 weeks1 more row
What is intensive phase in TB treatment?
For new TB cases, the treatment in intensive phase (IP) will consist of eight weeks of Isoniazid, Rifampicin, Pyrazinamide and Ethambutol in daily dosages as per four weight band categories. There will be no need for extension of IP.
Is TB curable in 3 months?
After taking TB medicine for several weeks, a doctor will be able to tell TB patients when they are no longer able to spread TB germs to others. Most people with TB disease will need to take TB medicine for at least 6 months to be cured.
How long is latent TB treatment?
CDC and the National Tuberculosis Controllers Association (NTCA) preferentially recommend short-course, rifamycin-based, 3- or 4-month latent TB infection treatment regimens over 6- or 9-month isoniazid monotherapy. Short course regimens include: Three months of once-weekly isoniazid plus rifapentine (3HP)
How many months is the treatment regimen for Category 2 TB patient?
The preferred continuation-phase regimen is four months of rifampicin and isoniazid (4RH) administered daily or three times weekly.
Why has it become more difficult to treat TB over time?
Most of the time TB can be cured with antibiotics. If you have TB, you will need to take several drugs. This is because there are many bacteria to be killed. Taking multiple drugs also helps to prevent the bacteria from becoming drug resistant and, thus, much more difficult to cure.
Why is treatment for TB generally continued long term after the infection appears to be wiped out?
tuberculosis to other persons. To ensure that these goals are met, TB disease must be treated for at least 6 months and in some cases even longer. Most of the bacteria are killed during the first 8 weeks of treatment; however, there are persistent organisms that require longer treatment.
Why does Mycobacterium tuberculosis grow slow?
Conversely, MTBs live long, are quite tolerant to different environments, and grow so slowly that their duplication time exceeds 18 hrs. The duplication time of mycobacterium leprae is even longer, so that all the cultivation efforts have failed.
How long does it take to treat TB?
Current WHO and national TB programme guidelines for TB treatment recommend two months of intensive, directly observed treatment with four drugs - isoniazid, rifampicin, ethambutol and pyrazinamide. Treatment then continues with either four months of rifampicin and isoniazid, or six months of isoniazid and ethambutol. However, the two continuation phase regimens have never been compared in a randomised study.
How long after treatment do you get unfavourable outcomes?
A Kaplan-Meier analysis of time to unfavourable outcome showed that as time went on, the risk of an unfavourable outcome among patients who received an eight month treatment regimen grew. Two and a half years after the beginning of treatment 5% of the six month treatment group had experienced an unfavourable outcome, compared to 10% of the eight month / daily induction treatment group and 15% of the eight month / three times weekly induction treatment group. Almost all unfavourable outcomes in the six month treatment group occurred during the first 18 months after treatment began, but continued to accumulate throughout the follow-up period in the eight month treatment groups.
How often is rifampicin given?
In South Africa's National TB Control Programme, for example, some treatment centres carry out TB treatment using a five month continuation phase in which isoniazid and rifampicin are given three times a week. Other centres give rifampicin and isoniazid five times a week during the four month continuation phase, and also give the induction regimen for five days out of seven during the first two months.
What is treatment failure?
Treatment failure was defined as a positive sputum culture at the end of treatment or a relapse after the end of treatment (defined as a culture of 20 or more colonies or initiation of treatment for relapse). Patients with one culture of 20 to 100 colonies followed by a negative culture and no new treatment were not defined as cases of relapse.
Does antiretroviral therapy help with TB?
Treatment advocates argue that antiretroviral therapy has provided other models that seem highly effective at encouraging adherence, and that national programmes could step up community-based adherence support for TB treatment if they invest in community-based treatment literacy programmes and building a cadre of community TB treatment supporters.
Who designed the study on Tuberculosis and Lung Disease?
The International Union Against Tuberculosis and Lung Disease and the United Kingdom Medical Research Council designed a study to answer two questions:
Does isoniazid compromise outcomes?
Baseline resistance to isoniazid did not compromise outcomes in the six month treatment group, but did compromise outcomes in the eight month treatment groups, where 31% of those with reduced isoniazid sensitivity had unfavourable outcomes compared to 7% of those with isoniazid sensitivity.
How long do you have to take TB medicine?
But TB bacteria die very slowly, and so the drugs have to be taken for several months. Even when a patient starts to feel better they can still have bacteria alive in their body. So the person needs to keep taking the drugs until all the bacteria are dead.
How long does TB treatment last?
For new patients with presumed drug susceptible pulmonary TB, the World Health Organisation (WHO) recommends that they should have six months of treatment. This consists of a two month intensive phase followed by a four month continuation phase.
What are the best drugs for TB?
The drugs that a patient should take depends on whether the patient has ever had TB treatment before. If the patient has never had treatment before then it can be assumed that the bacteria in the patient's body will respond, and be sensitive to all the TB drugs. So the patient can then be given the following drugs: 1 Isoniazid 2 Rifampicin 3 Pyyrazinamide 4 & Ethambutol.
Why does TB treatment fail?
It is often suggested that TB treatment fails because a patient doesn’t take their TB drugs correctly. However there can be a number of different reasons for TB treatment failure. It is certainly true that if a patient doesn’t take their TB drugs properly that this can lead to the development of drug resistant TB.
What is the responsibility of a doctor for TB?
A patient must take their drugs properly. But it is also the responsibility of the doctor to make sure that the patient has the correct drugs. The doctor must also explain to the patient how to take the drugs correctly. In many countries there are "alternative" medicines available.
How many drugs are there for TB?
There are more than twenty drugs available for TB treatment. Which ones have to be taken depends on the circumstances of the patient. If you are having TB treatment (sometimes known as antitubercular treatment or ATT), then this should always be supervised by an experienced doctor or other health person.
What happens if you take only one or two TB drugs?
If only one or two TB drugs are taken then only some of the bacteria may be killed. They may then become resistant to the TB drugs which then don't work. If the person becomes sick again then different TB drugs called second line drugs may be needed.
What is the first line of anti-TB drugs?
Of the approved drugs, the first-line anti-TB agents that form the core of treatment regimens are: isoniazid (INH), rifampin (RIF), ethambutol (EMB), and. pyrazinamide (PZA). Regimens for treating TB disease have an intensive phase of 2 months, followed by a continuation phase of either 4 or 7 months. The continuation phase should be extended ...
When should sputum be collected for TB?
Sputum specimens for microscopic examination and culture should be obtained from patients diagnosed with TB disease at a minimum of monthly intervals until two consecutive specimens are negative on culture. It is critical to obtain a sputum specimen at the end of the intensive phase (2 months) to determine if the continuation phase should be extended. In addition, it is essential that patients have clinical evaluations at least monthly to identify possible adverse effects of the anti-TB medications and to assess adherence. All patients with TB disease should have counseling and testing for HIV.
What is a DOT in TB?
DOT is a strategy in which a health care worker or another designated person watches the TB patient swallow each dose of the anti-TB drugs. All patients taking drugs fewer than 7 days per week (e.g., 1, 2, 3, or 5 days a week) must receive DOT.
How is treatment completion determined?
Treatment completion is determined by the number of doses ingested over a given period of time. Although basic TB regimens are broadly applicable, there are modifications that should be made under special circumstances (i.e., HIV infection, drug resistance, pregnancy, or treatment of children).
Is TB a public health function?
Treating tuberculosis (TB) disease benefits not only the individual patient but the community as a whole.Thus, any health care provider undertaking treatment of a patient with TB, whether a public health or private practitioner, is assuming a public health function that includes the responsibility for not only prescribing an appropriate regimen but also ensuring the patient’s adherence to the regimen until treatment is completed.
Can INH be used for HIV?
HIV-negative Persons. A continuation phase of once-weekly INH and rifapentine can be used for HIV-negative patients who do not have cavities on the chest film and who have negative acid-fast bacilli (AFB) smears at the completion of the intensive phase of treatment.
What is the treatment for tuberculosis?
Tuberculosis treatment is aimed at curing and rapidly reducing disease transmission. For this to occur, the drugs used should be able to reduce the bacillary population rapidly (interrupting transmission); prevent selection of naturally resistant strains (avoiding the emergence of drug resistance during therapy); and sterilize the lesion (preventing disease relapse).1
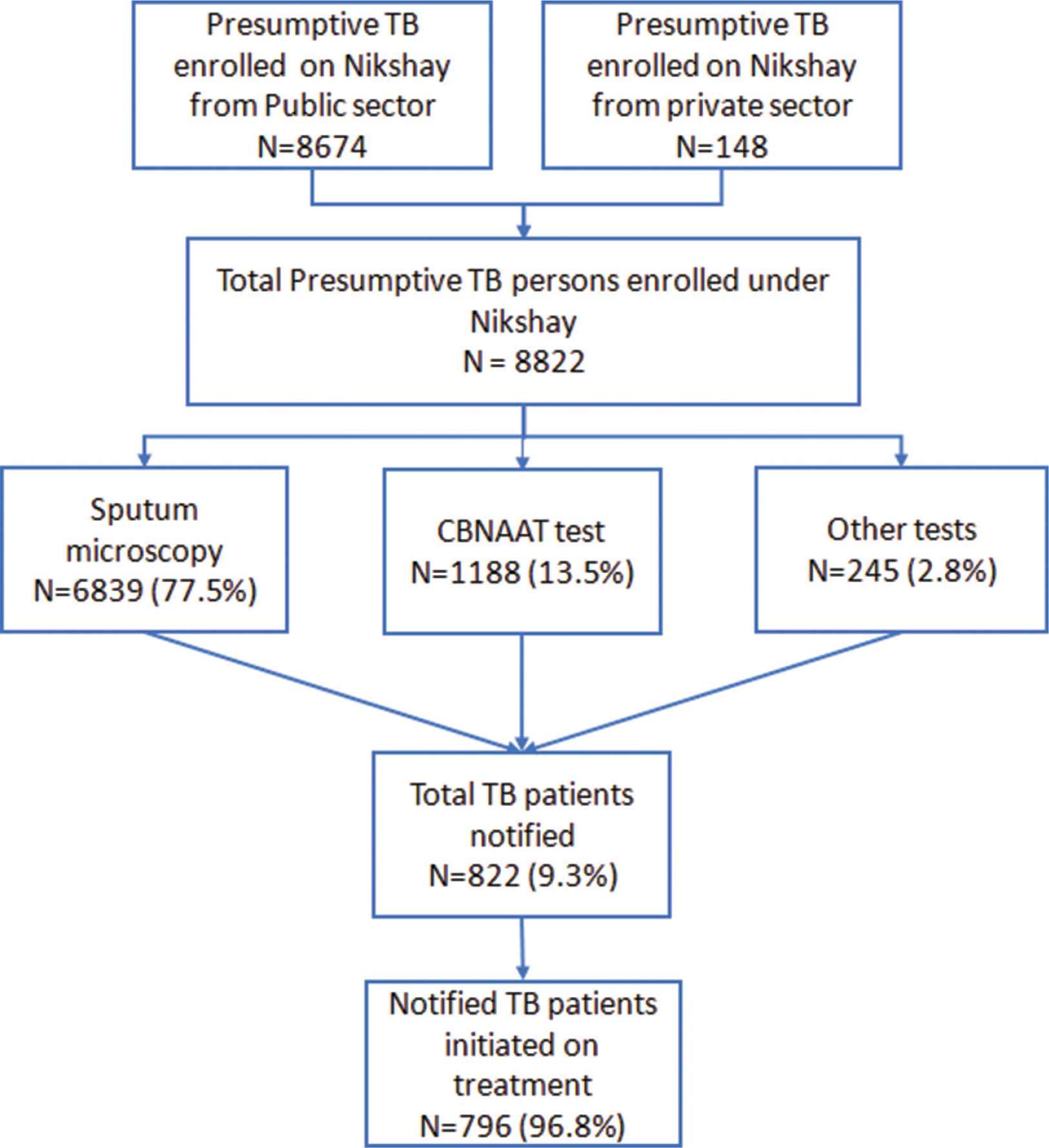
What is the basis for identification of tuberculosis cases?
Identification of tuberculosis cases on the basis of sputum smear microscopy among patients with respiratory symptoms
What is a tuberculosis control program?
A system for reporting and assessment of treatment results for each patient and for the tuberculosis control program as a whole
Why is tuberculosis a challenge?
Tuberculosis treatment remains a challenge due to the need to consider, when approaching it, the context of individual and collective health. In addition, social and economic issues have been shown to be variables that need to be considered when it comes to treatment effectiveness. We conducted a critical review of the national and international literature on the treatment of tuberculosis in recent years with the aims of presenting health care workers with recommendations based on the situation in Brazil and better informing decision-making regarding tuberculosis patients so as to minimize morbidity and interrupt disease transmission.
How long can a direct smear be extended?
Patients whose direct smears show few organisms at 5 or 6 months of treatment, alone , as long as there is clinical and radiological improvement-treatment can be extended for an additional 3 months, at which period cases should be redefined or closed
How long does it take to treat TB?
As a general rule, the principles used for the treatment of pulmonary TB disease also apply to extrapulmonary forms of the disease. A 6-month treatment regimen is recommended for patients with extrapulmonary TB disease, unless the organisms are known or strongly suspected to be resistant to the first-line drugs. If PZA cannot be used in the initial phase, the continuation phase must be increased to 7 months. The exception to these recommendations is central nervous system TB, for which the optimal length of therapy has not been established but some experts recommend 9 to 12 months. Most experts do recommend corticosteroids to be used as additional therapy for patients with TB meningitis and pericarditis. Consultation with a TB expert is recommended.
How long is the TB continuation phase?
The continuation phase of treatment is given for either 4 or 7 months. The 4-month continuation phase should be used in patients with uncomplicated, noncavitary, drug-susceptible TB, if there is documented sputum conversion within the first 2 months. The 7-month continuation phase is recommended only for
What are the four drugs that are included in the initial treatment regimen?
Four drugs— INH, RIF, PZA, and EMB — should be included in the initial treatment regimen until the results of drug-susceptibility tests are available. Each of the drugs in the initial regimen plays an important role. INH and RIF allow for short-course regimens with high cure rates. PZA has potent sterilizing activity, which allows further shortening of the regimen from 9 to 6 months. EMB helps to prevent the emergence of RIF resistance when primary INH resistance is present. If drug-susceptibility test results are known and the organisms are fully susceptible, EMB need not be included. For children whose clarity or sharpness of vision cannot be monitored, EMB is usually not recommended except when the risk of drug resistance is high or for children who have “adult-type” (upper lobe infiltration, cavity formation) TB disease.
What is the recommended treatment regimen based on?
The recommended treatment regimens are based, in large part, on evidence from clinical trials and are rated on the basis of a system developed by the U.S. Public Health Service (USPHS) and the Infectious Diseases Society of America (IDSA) (Table 6.3).
How to educate patients about TB?
Educating patients about TB disease helps ensure their successful completion of therapy. Health-care providers must take the time to explain clearly to patients what medication should be taken, how much, how often, and when. Patients should be clearly informed about possible adverse reactions to the medications they are taking and when to seek necessary medical attention. Providing patients with the knowledge they need regarding the consequences of not taking their medicine correctly is very important. In addition, patients should be educated about infection control measures and potential need for isolation (Table 6.1). HIV testing and counseling is recommended for all patients with TB disease in all health-care settings. The patient must first be notified that testing will be performed. The patient has the right to decline HIV testing and counseling (opt-out screening).
What are the drugs that treat TB?
Food and Drug Administration (FDA) for the treatment of TB disease (Table 6.2). In addition, the fluoroquinolones (levofloxacin, moxifloxacin, and gatifloxacin), although not approved by the FDA for TB disease, are commonly used to treat TB disease caused by drug-resistant organisms or for patients who are intolerant of some first-line drugs. Rifabutin, approved for use in preventing Mycobacterium avium complex disease in patients with HIV infection but not approved for TB disease, is useful for treating TB disease in patients concurrently taking drugs that interact with rifampin (e.g., certain antiretroviral drugs). Amikacin and kanamycin, nearly identical aminoglycoside drugs used in treating patients with TB disease caused by drug-resistant organisms, are not approved by the FDA for treatment of TB.
How long does it take to develop a TB control plan?
For each patient with newly diagnosed TB disease, a specific treatment and monitoring plan should be developed in collaboration with the local TB control program within 1 week of the presumptive diagnosis. This plan should include:
What is the best treatment for TB?
A four-drug regimen with INH, RIF, pyrazinamide (PZA), and SM or EMB is preferred for the initial, empiric treatment of TB (Tables 1,2). When adherence with the regimen is assured, such as with directly observed therapy (DOT), the four-drug regimen is highly effective even for INH-resistant organisms (7). Based on the prevalence and characteristics of drug-resistant organisms, at least 95% of patients will receive an adequate regimen (at least two drugs to which their organisms are susceptible) if this four-drug regimen is used at the beginning of therapy (CDC, unpublished data). Even with susceptible organisms, sputum conversion is accomplished more rapidly from positive to negative with a four-drug regimen than with a three-drug regimen of INH, RIF, and PZA (8). DOT is more easily managed with the four-drug regimen since it can be administered intermittently 3 times/week from the beginning of therapy (7). The four-drug regimen also can be administered 2 times/week following a 2-week induction phase of daily therapy (9). Finally, a patient who is treated with the four-drug regimen, but who defaults therapy is more likely to be cured and not relapse when compared with a patient treated for the same length of time with the three-drug regimen.
Why do we need multiple drugs for TB?
Because administration of a single drug often leads to the development of a bacterial population resistant to that drug, effective regimens for the treatment of TB must contain multiple drugs to which the organisms are susceptible. When two or more drugs are used simultaneously, each helps prevent the emergence of tubercle bacilli resistant to the others. However, when the in vitro susceptibility of a patient's isolate is not known -- which is generally the case at the beginning of therapy -- selecting two agents to which the patient's isolate is likely to be susceptible can be difficult. Improper selection of drugs for the treatment of drug-resistant TB (i.e., providing only one drug to which most organisms are susceptible) may subsequently result in the development of additional drug-resistant organisms.
How many TB cases were resistant to INH and RIF in 1991?
Based on surveys of all TB cases reported to CDC during the first quarter of 1991, cases of TB resistant to one or more drugs were reported from all 10 Health and Human Services/Public Health Service regions of the United States. Moreover, during the period 1982-1986, 0.5% of new TB cases were resistant to both INH and RIF, whereas preliminary analysis of data for the first quarter of 1991 suggests that this proportion was about 3%. Among recurrent cases, 3% were resistant to both drugs during the period 1982-1986, compared with 6.9% in 1991.
How does mycobacterium tuberculosis become drug resistant?
Mycobacterium tuberculosis becomes drug resistant through random, spontaneous genetic mutation. The proportion of naturally occurring resistance has been established for several of the primary anti-TB drugs: RIF, 1/108; INH and streptomycin (SM), 1/106; and ethambutol, (EMB) 1/104. Assuming that the mutations are independent, the likelihood of an organism spontaneously developing resistance to more than one drug is the product of probabilities; for example, the probability of INH and RIF resistance occurring in the same organism is 1/108 times 1/106 (1/1014). Because the total number of bacilli in an infected person, even with advanced cavitary disease, does not approach this number (1014), spontaneous evolution of MDR tubercle bacilli occurs infrequently.
When should PZA be discontinued?
Where the prevalence of drug resistance is sufficiently substantial to justify starting all patients on the four-drug regimen (i.e., a prevalence of INH resistance greater than or equal to 4%), PZA should be discontinued at 8 weeks, but EMB or SM should be continued (along with INH and RIF) for a total of 6 months. Immunosuppressed Patients
Why is there an excess number of cases of TB?
The excess number of cases is due to many factors, including the human immunodeficiency virus (HIV) epidemic, a deterioration in the health-care infrastructure, and increases in the number of cases among foreign-born persons . The recent emergence of drug-resistant TB also has become a serious concern.
When is in vitro susceptibility of a patient's isolate not known?
However, when the in vitro susceptibility of a patient's isolate is not known -- which is generally the case at the beginning of therapy -- selecting two agents to which the patient's isolate is likely to be susceptible can be difficult.
How long does it take to cure pulmonary TB?
This phase of treatment usually consists of INH and RIF for four months (16 to 18 weeks) to complete a total of six months of treatment, since most uncomplicated pulmonary TB patients become culture-negative within two weeks. If smears or cultures remain persistently positive, at least six months of therapy must be completed post culture conversion to negative, resulting in treatment duration of more than six months.
How is extrapulmonary TB managed?
In general, extrapulmonary TB (see Table 3-2, page 3-2, for clinical manifestations of extrapulmonary TB) should be managed according to the principles and drug regimens outlined for pulmonary disease. In contrast to pulmonary TB, diagnosis of extrapulmonary TB is more often made on clinical grounds without culture confirmation; thus, response to treatment often must be judged on the basis of clinical improvement. In situations where culture confirmation has been made, clinical follow-up is critical because it may be difficult to obtain follow-up specimens.
What is Medi-Cal for tuberculosis?
Eligibility for Medi-Cal should be determined for all patients as a means of facilitating care for related medical conditions during treatment for tuberculosis and to provide reimbursement to the County for the cost of care for outpatient services.
What is TB control program?
The TB Control Program (TBC) provides incentives and enablers to homeless and other indigent TB class 3 and class 5 individuals in an effort to facilitate treatment completion. Housing, meals, transportation, and substance abuse rehabilitation are available. Incentives and enablers should be used in situations where adherence to the TB medication regimen may be difficult for the individual. The health center clinician and staff should determine which eligible individuals should receive these services. The Incentive and Enabler Project Procedure Manual details eligibility and provisions and is available from TBC (see Appendix J, Incentives and Enablers Project Overview).
What is retreatment TB?
Retreatment cases are defined as TB cases who have completed an adequate course of TB drug therapy and remained bacteriologically negative for at least one year but subsequently develop signs of relapse with positive bacteriology. This is in contrast to patients who are treatment failures; that is, those cases whose sputa have not converted to negative despite four or more months of therapy or who initially improve, but then worsen clinically or bacteriologically despite continuation of therapy. Management of treatment failure is discussed in Chapter Five.
What is the standard of treatment for MDR-TB patients in LAC?
The standard of treatment of MDR-TB patients in LAC requires an automatic consultation with TBC. The MDR-TB Surveillance Unit collects and reviews MDR-TB patient data, which are then presented to the TBC physician staff. A written treatment plan with drug dosages and follow-up recommendations will be provided. The TB Control Program MDR-TB Surveillance Unit must approve any change in treatment. No changes are to be made prior to consultation with the MDR-TB Surveillance Unit except discontinuing medication because of serious drug side effects. Changes will be approved in writing only.
Can HIV patients discuss treatment options?
The complexities of management of HIV-infected individuals with TB make it impossible to discuss treatment options for all situations. New developments in the field of HIV treatment make it necessary to continually update and revise specific guidelines relating to management of TB in HIV-infected persons. Thus, care for such individuals must be done by or in consultation with experts familiar in the management of both TB and HIV disease.

Introduction
Recommended Regimens
- At the end of the two month intensive treatment phase sputum samples were available for 93% of patients who had provided samples within two weeks of the due date. Negative cultures were significantly fewer in the three times weekly treatment group: 77% of the three times weekly group had negative cultures, compared to 85% of patients who received d...
Hiv-Negative Persons
Case Management
Follow-Up Evaluations
For More Information
- A continuation phase of once-weekly INH and rifapentine can be used for HIV-negative patients who do not have cavities on the chest film and who have negative acid-fast bacilli (AFB) smears at the completion of the intensive phase of treatment.