What are the treatment goals when treating urinary tract infection (UTI)?
The treatment goals when treating urinary tract infection (UTI) include: 1. Eradication of infecting organism 2. Relief of symptoms 3. Prevention of recurrence of the UTI 4. All of the above 4. All of the above Sally is a 16-year-old female with a urinary tract infection.
What factors should be considered when making treatment decisions for UTI treatment?
Additional considerations that should factor into the treatment decision include patient allergies, recent antibiotic exposure, recent prior urine culture results, drug interactions, contraindications, cost and other patient factors, such as renal status.
What is included in the evaluation of urinary tract infection (UTI)?
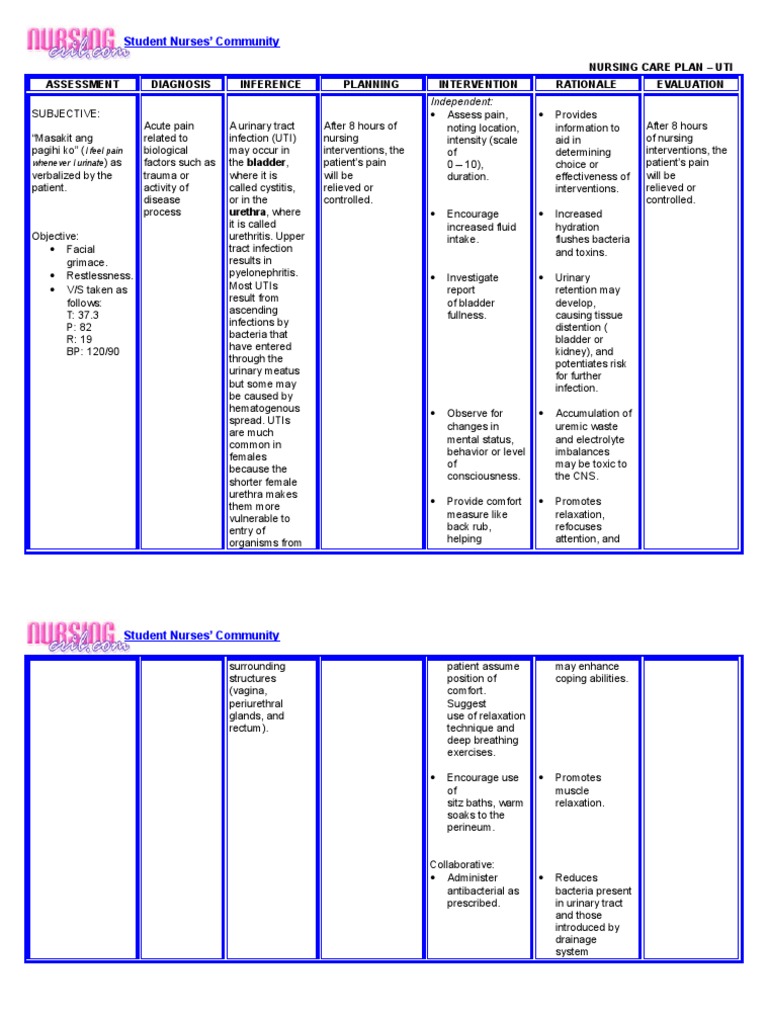
A history of signs and symptoms related to UTI is obtained from the patient with a suspected UTI. Assess changes in urinary pattern such as frequency, urgency, or hesitancy. Assess the patient’s knowledge about antimicrobials and preventive health care measures.
How to treat chronic and recurrent UTI?
Different methods are practiced to treat and prevent chronic and recurrent UTI, i.e., taking antibiotics, bioactive natural foods, using probiotics, and maintaining good personal hygiene, but still, they are yet to be addressed successfully. As UTI is generally caused by bacteria, they are most frequently treated with antibiotics.
What antimicrobials are used for cystitis?
Appropriate antimicrobials for the treatment of cystitis include trimethoprim-sulfamethoxazole (TMP-SMX), nitrofurantoin, fluoroquinolones, or cephalosporins. Some patients may require a urinary analgesic such as oral phenazopyridine, which is useful to relieve discomfort due to severe dysuria. Related Questions:
What is the best treatment for gram negative bacteria?
Oral therapy with an empirically chosen antibiotic that is effective against gram-negative aerobic coliform bacteria, such as Escherichia coli, is the principal treatment intervention in patients with lower urinary tract infections.
What is a UTI?
Urinary tract infections (UTIs) are common, recurrent infections that can be mild to life-threatening. The continued emergence of antibiotic resistance, together with our increasing understanding of the detrimental effects conferred by broad-spectrum antibiotic use on the health of the beneficial microbiota of the host, has underscored the weaknesses in our current treatment paradigm for UTIs. In this Review, we discuss how recent microbiological, structural, genetic and immunological studies have expanded our understanding of host-pathogen interactions during urinary tract pathogenesis. These basic scientific findings have the potential to shift the strategy for UTI treatment away from broad-spectrum antibiotics targeting conserved aspects of bacterial replication towards pathogen-specific antibiotic-sparing therapeutics that target core determinants of bacterial virulence at the host-pathogen interface.
What percentage of antibiotics are written for UTI?
Given that 9% of all antibiotic prescriptions in the ambulatory setting in the United States are written for the treatment of UTI, UTIs are at the forefront of the antibiotic resistance problem 139. Thus, there is an urgent need to develop antibiotic-sparing therapeutics for the treatment of UTI.
What causes UTIs in catheterized patients?
Although short-term community- and catheter-associated UTIs are mostly caused by monomicrobial infections, most CAUTIs in patients catheterized for long periods (>30 days) are polymicrobial in nature 132, 133. p. mirabilis, a Gram-negative bacterium that is nearly ubiquitous in soil and water, is a common constituent of CAUTI polymicrobial communities in chronically catheterized patients 133, 134. p. mirabilis uses various canonical virulence factors to establish infection in the bladder, including flagella and adhesive mannose-resistant Proteus-like MR/P fimbriae 135 ( Fig 3 ). In addition, P. mirabilis expresses high levels of urease, an enzyme that can hydrolyze urea to ammonia and raise the pH of urine to facilitate the formation of kidney stones 135. Although carriage of this enzyme is not uncommon in uropathogens, P. mirabilis urease activity generates a substantially higher urinary pH than any of its uropathogenic counterparts, enabling the formation of crystalline biofilms that provide a protective niche during antibiotic treatment, promoting recurrence 136. Recent work has revealed that, like UPEC, P. mirabilis invades the superficial umbrella cells of the bladder and forms IBCs in the urothelium 137.
What causes urinary tract infections?
Urinary tract infections (UTIs) are common infections caused predominantly by uropathogenic Escherichia coli (UPEC), which cause approximately 80% of UTIs. The annual incidence of physician-diagnosed UTIs in the United States is greater than 10% for females and 3% for males, and more than 60% of females will be diagnosed with a UTI in their lifetime 1, 2. Individual risk for infection depends on various factors, including age, sexual activity, family history, medical comorbidities and an individual history of UTI ( Box 1) 3. Recurrent UTIs (rUTIs; defined as three or more UTIs during a 12 month period 4) contribute greatly to the incidence and morbidity rates of UTI, as more than 30% of women will suffer from a subsequent infection within 12 months of resolution of initial symptoms despite appropriate antibiotic therapy 5. UTIs are becoming increasingly difficulty to treat owing to the rapid spread of drug resistance among Gram-negative organisms, including UPEC 6.
What bacteria are responsible for nosocomial cauti?
Enteroccocus faecalis and E. faecium are Gram-positive bacteria responsible for up to 17% of nosocomial CAUTIs 110, 113. Over 85% of E. faecium and 7% of E. faecalis clinical CAUTI isolates tested were found to be resistant to vancomycin 113. Using a mouse foreign-body implantation model of UTI ( Supplementary figure S1 ), it was found that Enterococci utilize endocarditis- and biofilm-associated pili (Ebp) to form biofilms on catheters and overcome the neutrophil-mediated immune response 119 ( Fig 3 ). Ebp pili are tipped with a fibrinogen-binding adhesin known as EbpA, which binds to the fibrinogen coating the catheter. Mutation of the N-terminal metal-ion-dependent fibrinogen-binding domain of the EbpA adhesin, or blockade with antibodies raised against the N-terminal domain of EbpA, prevents bacterial adhesion to fibrinogen-coated catheters in vitro and in mouse models of infection 120. Enterococci also use fibrinogen as a nutrient source, enabling their growth in urine 120. Enterococcal virulence is dependent on two secreted proteases, GelE and SprE, which are upregulated during infection to cleave the α-, β- and γ-chains of fibrinogen to potentiate biofilm formation ( Fig 3) 122. This provides further evidence that Enterococcus species utilize fibrinogen as both a binding platform and food source during biofilm formation and growth. Activation of SprE by host proteases was further shown to promote bacterial dissemination in the kidneys, whereas inhibition of either host or bacterial proteases was able to curb bacterial dissemination 120. Ebp pili are also important for cell-cell aggregation and interspecies gene transfer, facilitating the spread of genetic elements that encode antibiotic resistance and other virulence factors 123.
What is the ultimate reservoir for UPEC?
The gastrointestinal tract is the ultimate reservoir for UPEC, and FimH and has been shown to have a critical role in maintaining colonization of this habitat in mice. Depletion of this reservoir within a given host would be expected to reduce the rate of recurrent UTIs.
What is the role of P pili in pyelonephritis?
P pili bind globosides in the kidney and are essential for progression to pyelonephritis. Biophysical studies performed on type 1 pili revealed the importance of conformational dynamics in the adhesin and pilus rod during infection (right panel).
Associated Data
All data generated or analyzed during this study are included in this published article.
Abstract
The recurrence of the urinary tract infections (UTI), following the antibiotic treatments suggests the pathogen’s resistance to conventional antibiotics. This calls for the exploration of an alternative therapy.
Background
Urinary tract infection (UTI) is a condition when any part of the urinary tract (urethra, bladder, ureter, and kidney) gets infected with bacteria or occasionally with fungus that evades the host defense barrier and colonize the urinary tract.
Methods
Intense review of literature on the prevalence, mechanism of urinary tract infection, risk factors, preventive measures, and natural therapeutics for UTI were carried out using different databases like Google, Pubmed, and Sciencedirect.
Botanicals used for UTI
Therapeutic botanicals are defined as plants and their products with medicinal value. Indigenous plants are used for various ailments since time immemorial by mankind and probably we had learned this art from animals, since they have the inherent ability to use natural products for their different health ailments.
Botanicals with anti-uropathogenic activity
Few Jordanian plants were reported to have antibiotic resistance-modifying activity against MDR E. coli. Especially, methanol extracts of the plant parts improved the effects of cephalexin, doxycycline, neomycin, chloramphenicol, and nalidixic acid against both the standard and resistant strains of E. coli. Extracts of Anagyris foetida L.
Cranberry: a potent uroprotective agent
For centuries, cranberries have been used as a treatment for urinary tract diseases and its antibacterial activity was reported long back [ 60 ].
What is the best treatment for UTI?
Acute pharmacologic therapy. The ideal medication for the treatment of UTI is an antibacterial agent that eradicates bacteria from the urinary tract with minimal effects on fecal and vaginal flora. Long-term pharmacologic therapy.
Why is early recognition of UTI important?
Early recognition of UTI and prompt treatment are essential to prevent recurrent infection and the possibility of complications. ADVERTISEMENTS. Renal failure. UTIs that are not treated promptly could spread in the entire urinary system and become the cause of renal failure.
How to prevent urethra infection?
Perineal hygiene. After each bowel movement, clean the perineum and urethral meatus from front to back to reduce concentrations of pathogens at the urethral opening. Increase fluid intake.
How common is UTI?
Urinary tract infection cases are widespread around the world and affect both the young and the old. UTI is the second most common infection in the body. Most cases of UTI occur among women; one out of five women in the United States will develop UTI during her lifetime.
What is a negative urine culture?
2. Answer: C. Cloudy urine. C: Cloudy urine shows infection because of the bacteria that has invaded the urinary tract. A: A negative urine culture is a sign that there is no infection.
What could introduce bacteria into the urinary tract?
Instrumentation of the urinary tract. Catheterization or cystoscopy procedures could introduce bacteria into the urinary tract. Obstructed urinary flow. Abnormalities in the structure of the urinary tract could obstruct the flow of the urine and result in inability to empty the bladder completely.
What happens when bacteria attach to the epithelium of the urinary tract?
The bacteria attach to the epithelium of the urinary tract and colonize it to avoid being washed out with voiding. Evasion. The defense mechanisms are then evaded by the host. Inflammation. As the defense mechanisms react to the bacteria, inflammation starts to set in as well as other signs of infection.
