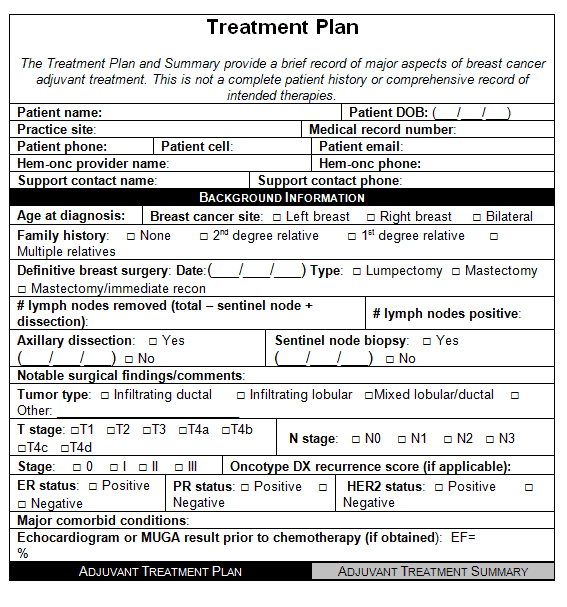
A treatment plan is simple but specific. Although treatment plans vary, a treatment plan template or form generally contains the following fields: Patient information: At the top of the treatment plan, the counselor will fill in information such as the patient’s name, social security number, insurance details, and the date of the plan.
Full Answer
What are some examples of treatment plans in occupational therapy?
Examples of Treatment Plans 1 OT will review the handout with the pt on a one-to-one basis. 2 OT will lead a questions and answers session after reviewing the handout. 3 OT will request that the pt review the handout in order to verbally recite the safety techniques explained in the handout.
How to write a treatment plan for mental health?
1 Defining the problem or ailment 2 Describing the treatment prescribed by the health/ mental health professional 3 Setting a timeline for treatment progress (whether it’s a vague timeline or includes specific milestones) 4 Identifying the major treatment goals 5 Noting important milestones and objectives
What is the treatment plan for each patient?
Each patient must have an individualized, goal and action-oriented treatment plan that is based upon information obtained in the assessment process .
Do I need a treatment plan for my therapist?
While treatment plans can prove beneficial for a variety of individuals, they may be most likely to be used when the person in therapy is using insurance to cover their therapy fee. In these cases, a therapist may be required to submit a treatment plan to the client’s insurance company.

What is occupational therapy goals examples?
1. Remembering a List – Restoring and maintaining memory are key goals for cognitive occupational therapy. 2. Learning Nonverbal Cues – For patients with cognitive impairments, such as autism, learning social cues is an important step along the path to developing meaningful relationships.
How do you write occupational therapy goals?
SMART stands for Specific, Measurable, Attainable, Relevant, and Time Based. By using this acronym as a guide, you can ensure your goals contain all the relevant information necessary. SMART goals are also universally used and easy for you, your client, and any other medical professionals involved to understand.
How do you write a good occupational therapy note?
Make sure to include:Observations of how the client is performing in a specific task.How the client is performing throughout their occupational therapy session.Details about specific interventions or therapeutic activities the client engaged in and their response.
What is an intervention plan in OT?
Intervention plan refers to a detailed proposal that outlines the anticipated treatment approach, methods, and goals to be employed during occupational therapy services. The intervention plan should also include appropriate discharge recommendations and referrals to other health professionals as needed.
How do you write smart goals in occupational therapy?
When choosing one of these goals, remember to make sure you plan them the SMART way.Specific – Know exactly what you want to accomplish.Measurable – Track your progress.Achievable – Outline the steps you will take to reach your goal.Relevant – Ensure the goal fits in with your current and upcoming needs.More items...
How do you write a measurable treatment goal?
2. Set SMART GoalsSpecific: Objectives need to be clear and specific, not general or vague. ... Measurable: Objectives need specific times, amounts or dates for completion so you and your patients can measure their progress.Attainable: Encourage patients to set goals and objectives they can meet.More items...•
How do I write an occupational therapy progress report?
The basics of an occupational therapy progress note template must include client-specific details (on each page), a review of what goals/actions were taken during the session by the client and the practitioner, and the practitioners' assessment of the client's actions, followed by corresponding updates, and ...
What is SOAP note format?
The SOAP format – Subjective, Objective, Assessment, Plan – is a commonly used approach to. documenting clinical progress. The elements of a SOAP note are: • Subjective (S): Includes information provided by the member regarding his/her experience and. perceptions about symptoms, needs and progress toward goals.
What kind of writing do occupational therapists do?
Four types of writing will be addressed: journal or reflective writing, developing fact sheets or handouts, technical writing specific to the profession, and scholarly writing of research papers (i.e., professional summaries, research papers, etc.).
What are the 5 general treatment approaches used in OT practice?
Provide examples of the type of OT services considered within each area. What are some nontraditional settings in which OT practitioner work? What are the five general treatment approaches used in occupational therapy practice?...Create/promote.establish, restore.maintain.modify.prevent.
What are the five different intervention approaches?
Use the framework intervention approaches to define the most appropriate focus for each domain listed below, using one or more of these five approaches: create/promote, establish/restore, maintain, modify, or prevent.
What is treatment planning?
Treatment planning is a team effort between the patient and health specialist. Both parties work together to create a shared vision and set attainable goals and objectives.
What is the third section of a treatment plan?
Problems and goals: The third section of the treatment plan will include issues, goals, and a few measurable objectives. Each issue area will also include a time frame for reaching goals and completing objectives. Counselors should strive to have at least three goals.
What information do counselors fill out?
Patient information: At the top of the treatment plan, the counselor will fill in information such as the patient’s name, social security number, insurance details, and the date of the plan. Diagnostic summary: Next, the counselor will fill out a summary of the patient’s diagnosis and the duration of the diagnosis.
What is a goal in a patient's life?
Both parties work together to create a shared vision and set attainable goals and objectives. A goal is a general statement of what the patient wishes to accomplish. Examples of goals include: The patient will learn to cope with negative feelings without using substances.
What are some examples of objectives?
Examples of objectives include: An alcoholic with the goal to stay sober might have the objective to go to meetings. A depressed patient might have the objective to take the antidepressant medication with the goal to relieve depression symptoms.
What is objective in a patient?
An objective, on the other hand, is a specific skill a patient must learn to reach a goal. Objectives are measurable and give the patient clear directions on how to act.
What is the role of model and technique in a treatment plan?
Treatment plans provide structure patients need to change. Model and technique factors account for 15 percent of a change in therapy. Research shows that focus and structure are critical parts of positive therapy outcomes. Goal-setting as part of a treatment plan is beneficial in itself. Setting goals helps patients:
About This Chapter
Review information about occupational therapy intervention and treatment planning processes using this informative chapter. This is a great resource you can use to supplement your class studies or prepare for professional certification exams.
1. Intervention Planning in OT: Models of Practice & Activity Selection
If you are thinking about helping a patient using occupational therapy, you are probably considering different aspects of intervention planning. This lesson discusses some procedures and theories that you might find helpful.
2. Occupational Therapy Process: Stages & Intervention
Understanding the different stages that someone goes through when they are referred for occupational therapy support can be very helpful. This lesson walks you through the steps from screening to intervention and discharge.
3. Factors Influencing Occupational Performance
If you're an occupational therapist, you might be wondering more about what makes some patients have certain strengths and weaknesses. This lesson discusses a variety of factors that can influence occupational performance.
4. Modifying Treatment Plans in OT: Methods & Examples
As an occupational therapist, you probably understand the importance of remaining flexible in your work. This lesson discusses what it might mean to modify a treatment plan for a patient in the context of OT.
5. Occupational & Physical Therapy: Vocabulary
There are tons of occupational and physical therapy techniques out there. While we can't go over all of them, we will define occupational and physical therapy as well as vocabulary related to them.
6. Interprofessional Communication & Collaboration in Healthcare
When healthcare teams work together, everyone benefits. In this lesson, you'll find out how to use effective communication to manage conflicts and support patient care within the interprofessional team.
Understanding OT Treatments
Rita has been working as an occupational therapist, someone who helps patients with fine motor control, core strength, and sensory integration as relevant to their daily, leisure, work, and educational activities, for ten years.
Monitoring Progress
First, Rita knows that it is crucial for her to monitor, or oversee, the progress of each of her patients over time. There are a few different ways that Rita does this.
Recognizing Indicators
By monitoring progress in this way, Rita is able to recognize indicators, or signs, that the treatment plan might no longer be relevant, and something needs to change.
Making Changes
Rita considers herself successful when she is able to take these different indicators to heart and sit down to make real changes in her approach to OT.
Subjective (S)
Each note should tell a story about your patient, and your subjective portion should set the stage.
Objective (O)
The objective section of your evaluation and/or SOAP note is often the longest. This is almost certainly the case in an evaluation.
Assessment (A)
The assessment section of your OT note is what justifies your involvement in this patient’s care.
Plan (P)
I once went to a CEU course on note-writing, and the course was geared toward PTs.
More resources for improving your documentation
I recognize that defensible documentation is an ever-evolving art and science, and have come across many useful resources that will help you keep your notes complete, yet concise. I highly recommend the following:
Conclusion
Documentation can get a bad rap, but I believe that OT practitioners are uniquely poised to write notes that are meaningful to other healthcare practitioners and patients alike.
Why are treatment plans important?
Treatment plans are important for mental health care for a number of reasons: Treatment plans can provide a guide to how services may best be delivered. Professionals who do not rely on treatment plans may be at risk for fraud, waste, and abuse, and they could potentially cause harm to people in therapy.
Why do people need treatment plans?
Treatment plans can also be applied to help individuals work through addictions, relationship problems, or other emotional concerns. While treatment plans can prove beneficial for a variety of individuals, they may be most likely to be used when the person in therapy is using insurance to cover their therapy fee.
What is HIPAA treatment plan?
Treatment Plans and HIPAA. The Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule grants consumers and people in treatment various privacy rights as they relate to consumer health information, including mental health information.
What is a mental health treatment plan?
Mental health treatment plans are versatile, multi-faceted documents that allow mental health care practitioners and those they are treating to design and monitor therapeutic treatment. These plans are typically used by psychiatrists, psychologists, professional counselors, therapists, and social workers in most levels of care.
What does a therapist do for Chris?
Therapist will provide psychoeducation on positive parenting and will support Chris in developing a concrete parenting plan. Therapist will provide materials for Chris to document the new house rules, rewards, and consequences system.
What is progress and outcomes?
Progress and outcomes of the work are typically documented under each goal. When the treatment plan is reviewed, the progress sections summarize how things are going within and outside of sessions. This portion of the treatment plan will often intersect with clinical progress notes.
Do you need a treatment plan for a 3rd party?
Treatment plans are required if you accept 3rd party reimbursement and are just good practice. They are a road map to treatment. They are fluid and are developed with the client/patient. Pretty much necessary if you are doing your job as a therapist.
SHOW-NOTES (transcript)
Hi, Patrick Martin here, and in this post I will be sharing with you how to create a CBT treatment plan and this is the second part of the clinical loop.
Create A Treatment Plan Using The S.M.A.R.T. Model
Alright, another acronym that can help us out complements the smart model, and this is known as the P.O.W.E.R. model.
Final Thoughts On Creating A Treatment Plan
So, when it comes to making measurable goals right, those objectives we can use some tools and counseling to help us do that.
Why do we need treatment plans?
Treatment plans can reduce the risk of fraud, waste, abuse, and the potential to cause unintentional harm to clients. Treatment plans facilitate easy and effective billing since all services rendered are documented.
What is a mental health treatment plan?
At the most basic level, a mental health treatment plan is simply a set of written instructions and records relating to the treatment of an ailment or illness. A treatment plan will include the patient or client’s personal information, the diagnosis (or diagnoses, as is often the case with mental illness), a general outline ...
What is the treatment contract?
Treatment Contract – the contract between the therapist and client that summarizes the goals of treatment. Responsibility – a section on who is responsible for which components of treatment (client will be responsible for many, the therapist for others)
What is the part of effective mental health?
Part of effective mental health treatment is the development of a treatment plan. A good mental health professional will work collaboratively with the client to construct a treatment plan that has achievable goals that provide the best chances of treatment success. Read on to learn more about mental health treatment plans, how they are constructed, ...
What is intervention in therapy?
Interventions – the techniques, exercises, interventions, etc., that will be applied in order to work toward each goal. Progress/Outcomes – a good treatment plan must include space for tracking progress towards objectives and goals (Hansen, 1996)
What is blended care in therapy?
Blended care involves the provision of psychological services using telecommunication technologies.
What is a goal in counseling?
Goals are the broadest category of achievement that clients in mental health counseling work towards. For instance, a common goal for those struggling with substance abuse may be to quit using their drug of choice or alcohol, while a patient struggling with depression may set a goal to reduce their suicidal thoughts.
Subjective
- First, Rita knows that it is crucial for her to monitor, or oversee, the progress of each of her patients over time. There are a few different ways that Rita does this. She always takes notes and keeps records of each session with her patients. In these notes, Rita jots down what activities she did, what the patient was and was not able to do, and ...
Objective
Assessment
Plan
- DO use the subjective part of the note to open your story
Each note should tell a story about your patient, and your subjective portion should set the stage. Try to open your note with feedback from the patient about what is and isn’t working about their therapy sessions and home exercise program. For example, you can say any of the following to … - DON’T go overboard with unnecessary details
Let’s admit it: we are storytellers, and we like to add details. But, we must admit we’ve all seen notes with way too much unnecessary information. Here are a few things you can generally leave out of your notes: 1. “Patient was seated in chair on arrival.” 2. “Patient let me into her home.” 3. “…
General Do’s and Don’ts For Documentation
- DO go into detail about your observations and interventions
The objective section of your evaluation and/or SOAP note is often the longest. This is almost certainly the case in an evaluation. This section should contain objective measurements, observations, and test results. Here are a few examples of what you should include: 1. Manual …
Example Outpatient Occupational Therapy Evaluation
- DO show clinical reasoning and expertise
The assessment section of your OT note is what justifies your involvement in this patient’s care. What you’re doing in this section is synthesizing how the story the patient tells combines with the objective measurements you took (and overall observations you made) during today’s treatmen… - DON’T skimp on the assessment section
The assessment section is your place to shine! All of your education and experience should really drive this one paragraph. And yet… We tend to just write: “Patient tolerated therapy well.” Or we copy and paste a generic sentence like this: “Patient continues to require verbal cueing and will …
More Resources For Improving Your Documentation
- DON’T get lazy
I once went to a CEU course on note-writing, and the course was geared toward PTs. It felt to me like most of the hour was spent talking about how important it is to make goals functional. But we OTs already know this; function is our bread and butter. So, why do many OTs insist on writing th… - DO show proper strategic planning of patients’ care
This section isn’t rocket science. You don’t have to write a novel. But you do need to show that you’re thinking ahead and considering how your patients’ care plans will change as they progress through treatment. Consider something like this: “Continue working with patient on toileting, whil…
Conclusion
- Your patient is the hero—and you are the guide. In every good story, there’s a hero and a guide. The patient is Luke Skywalker, and you are Yoda. I think as therapists, we tend to document only one part of the story. For example, we focus on the hero’s role: “Patient did such and such.” Or we focus on what we, the guide, bring with our skilled interventions: “Therapist downgraded, correct…